

A Better Way To Lockdown
In a hyper-connected world, "lockdowns" are an important tool to slow the spread of a highly contagious virus, however, their exact implementation might be improved with a simple change.

The Counterpoint is a newsletter that uses both analytic and holistic thinking to examine the wider world. My goal is that you find it ‘worth reading’ rather than it necessarily ‘being right.’ Expect regular updates on the SARS-CoV-2 pandemic as well as essays on a variety of topics. I appreciate any and all sharing or subscriptions.
[Editor’s Note: As a professional scientist, the currency of my trade is journal publications. Scientific papers always begin with an abstract, a one-paragraph summation of the entire argument. Basically, a quick way of determining if it is ‘worth reading.’ I’ve always liked this feature of scientific writing and will replicate it here and in future Counterpoint Essays.]
Abstract: SARS-CoV-2 was the first highly-fatal pandemic of the modern, hyper-connected world. Given the scale of both inter- and intra-connection, classic ‘movement restrictions’ were scaled from individual or city quarantines to nationwide lockdowns. Such levels of restrictions had never been attempted. While having the desired public health impact, they also caused economic damage, psychological pain, and societal strife. An honest assessment of their effectiveness, externalities, and exact implementation is needed. Different versions of the same interventions can alter that interventions’ outcome (think single-layer cloth masks vs KN95 or N95s, the ‘same’ intervention (masks) but the latter are much more effective). Given the certainty of future epidemics and pandemics, the United States needs to improve it’s pandemic response plan. New and creative implementations of ‘lockdowns’ may provide a positive public health impact with less negative side effects.
Local epidemics are essentially continuous throughout history and even global pandemics occur regularly. Within the last ~100 years, there was the 1918 H1N1 influenza (~17-100 million deaths), the 1958 H2N2 influenza (~1-4 million deaths), the 1968 H3N2 influenza (~1-4 million deaths), the 2009 H1N1 influenza (~300,000 deaths). And that’s just the influenzas!
Within the last twenty years, three separate novel coronaviruses have jumped from animals into humans: the 2003 SARS-CoV, the 2012 MERS-CoV, and the 2019 SARS-CoV-2. Fortunately, the exact biological characteristics of the first two allowed for better containment, limiting the death toll to ~1,000 each. Unfortunately, SARS-CoV-2 was both more transmissible and could be spread asymptomatically, vaulting it from local epidemic within Wuhan to an all-out global pandemic.
This preamble was a long-winded way of saying that the likelihood of another viral pandemic in the coming decades is essentially a certainty (in fact, we’re overdue for another influenza pandemic). Disease prevention and control has always been and always will be an important and ongoing problem and it is important that we learn from SARS-CoV-2 so that our response to the pandemic improves.
Non-pharmaceutical interventions were a critically important part of our response to SARS-CoV-2. In fact, before the first positive pharmaceutical clinical trials and the development of the vaccines, they were our only options to control the spread of SARS-CoV-2.
At the very initial stages of the pandemic, numerous governmental and public health offices judged “lockdowns,” or more broadly “movement restrictions,” to be a useful tool in containing the virus.
Of course, these were not new tools. The word "quarantine" originates from Venetian “quarantena,” or "forty days,” due to the 40-day isolation of ships and people practiced in the port as a measure of disease prevention. What was new was the scale of such restrictions. Never before had they been applied to entire nations or the globe (for example, in Albert Camus’ classic ‘The Plague,’ an entire city is quarantined, but no more).
There was a reason for this new scale of restriction. Following decades of globalization and industrialization, the world is both more inter-connected and intra-connected. During the 1918 influenza, neither international air travel nor the interstate highway system existed. If the level of restrictions were not scaled to match the the hyper-connectedness of the modern world, SARS-CoV-2 would’ve run rampant, crashing every hospital system in the world within weeks, just as it did Wuhan, Bergamo, and New York City.
In retrospect, the data suggests that such restrictions were effective at preventing and controlling viral spread. Below is the key figure from an analysis and ranking of non-pharmaceutical interventions published in Nature in November 2020. Numerous ‘movement restrictions’ (the yellow shaded interventions) were judged to have the largest decrease in R(t), a measure of viral spread.

While effective, that doesn’t mean that lockdowns aren’t without their downsides. Bluntly: lockdowns suck. More explicitly: lockdowns have profound economic and psychological side effects. Governments around the world provided massive monetary and fiscal stimulus to blunt the former, while individuals, families, and online communities sought to minimize the the later. These efforts ‘staunched the bleeding’ but both remain seriously wounded: the unemployment rate remains ~50% higher than pre-COVID and rates of mental health disorders, substance abuse, and suicide ideation were elevated throughout 2020.
The worst: we never really locked down (at least in the United States). Okay, perhaps the spring lockdowns could be considered true ones (read the list of 'essential businesses’ in Los Angeles’ spring stay-at-home order and decide for yourself). But after the initial weeks of lockdowns, mobility data suggests a fairly steady re-opening trend that topped out just slightly below normal for many areas.

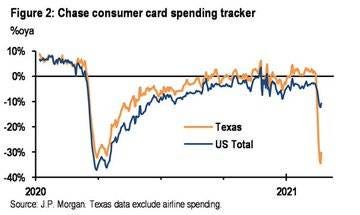
The mobility data correlates with credit card spending data from JP Morgan Chase (which also shows how severe the situation in Texas was during the polar vortex).
Below is a portion of quote from the CEO Tanger Factory Outlet Centers, an owner of malls, during the latest quarterly conference call. In the midst of record high daily deaths from COVID-19, “traffic was approximately 90% of prior year levels during the fourth quarter [of 2020].”
For a variety of political and sociological reasons, only half-hearted public health measures occurred within the United States. Consequently, we managed to achieve slight benefits (a minor reduction in viral spread) but with all of the pain (economic, psychological, and health consequences) With over 500,000 deaths and counting, we need to evaluate and improve our response so that we can prepare for the certainty of future pandemics.
Extended lockdowns did not work within the United States. But fault isn’t with the lockdown, but with the “extended.”
Instead of multi-week lockdowns being implemented at the judgement of political and public health leaders, after the spring lockdown, the United States should’ve implemented mandatory, nationwide lockdowns for the first seven days of every month, regardless of what the numbers were. Restrictions during the rest of the month would be minimal (mandatory masks and continued closure of high risk activities such as indoor dining, concerts, etc.) Everything else opens.
This may provide the same or better public health results with less negative externalities.
The “lockdown for the first seven days of every month” approach has numerous advantages.
It’s clear: “Stay at home the first seven days of the month,” is something that a child can understand.
It’s concise: No pages and pages of rules and regulations. No political lobbying by industries to be deemed essential. No “epidemiologists says parks and beaches are safe, why are they closed.” It’s ‘everything is closed the first seven days, everything is open the rest of the month.’ (With minor exceptions, like grocery, medical, and utilities remaining always open and indoor dining and concerts remaining always closed.)
It’s consistent: Families and business cannot plan for arbitrary lockdown and re-opening dates. If you operate a restaurant and case numbers are rising, should you place the next order for fresh produce, with the risk that it spoils during a new lockdown? Moreover, it eliminates the mixed-messaging from political leaders that are trying to balance the public health and economic concerns. Below is a what would be considered a ‘parody’ of Californian leaders, if only it weren’t perfectly true.
It’s fair: A pandemic is a ‘sinking ship’ moment; we’re all in this together. This is the “public” in “public health.” No (understandably) upset restaurant owners while movie sets operate next door. No stores, such as Gamestop, claiming to be essential. It’s ‘we’re all in this together, we all need to stay home the first seven days of every month.’ The more fair an intervention, the more likely it is to be followed; the more people that follow an intervention, the more effective it will be.
It’s balanced: By having short but clearly defined windows of ‘lockdown’ and ‘opening,’ you provide businesses with an economic outlet. Closed for seven days a month means they’re operating at ~75% monthly capacity. Combined with government stimulus, this should be enough to allow them to survive.
It’s proactive: Because political leaders are trying to balance the economic and societal concerns, they consider lockdowns a last resort. But given the nature of viral spread, managing a pandemic is more ‘steering an oil tanker’ than ‘racing a speedboat.’ Decisions need to be made weeks prior of any impact, yet time and time again, our leaders refused to make the hard choices. Over 2,000 Americans were dying per day before much of the nation reacted to the winter wave. In Los Angeles, ambulances were rationing oxygen and the county lifted air quality restrictions on crematories, yet malls remained open!
It’s proactive, part two: Rather than using extended lockdowns as a last resort to “crush the curve,” we should see them as regular speed bumps that slow exponential waves. Exponential waves aren’t a problem in the beginning (the 1 -> 2 -> 4 -> 8), they are are problem when they are left unchecked and allowed to continue (the 16-> 32 -> 64 -> 128). The below video went viral at the beginning of the pandemic. It made intuitive sense in regards to social distancing, but why not apply the same logic to lockdowns? The average incubation time for SARS-CoV-2 is 5.1 days and with peak transmission of the virus before and around the onset of symptoms. By getting everyone inside and isolated for the first seven days a month, you 1) allow symptomatic cases of COVID to be detected and 2) stop asymptomatic people from spreading.


In conclusion, I’ve proposed an alternate implementation of nationwide lockdowns. While optimistic of its potential benefit, it is not a panacea. No single intervention (other than universal vaccination) can control a highly contagious virus once it is endemic within a country. Each and every non-pharmaceutical intervention used during the SARS-CoV-2 pandemic, ranging from masks to lockdowns, needs to be evaluated and analyzed for potential improvement.
If you enjoyed The Counterpoint, please share, subscribe, or comment, below.