

SARS-CoV-2 Miscellaneous Update
Reviewing January predictions, why are caseloads decreasing so drastically, an update on vaccines and variants, and comments on viral evolution

Reviewing January predictions
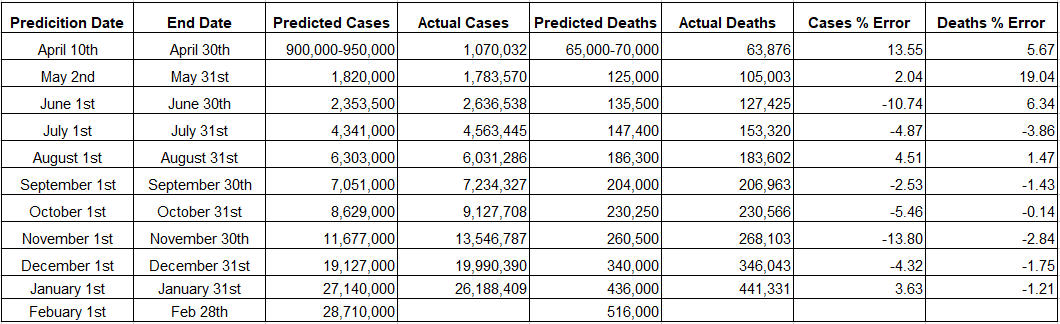
I predicted that at the end of January there would be 27,140,000 confirmed cases and 436,000 confirmed deaths from COVID-19 in the United States. On the morning of February 1st, there were 26,188,409 confirmed cases and 441,331 confirmed deaths.
The cases prediction was made with great uncertainty. On Jan 1st, cases were still climbing from the Christmas slowdown but their growth was slowing, signaling a potential peak and reversal in January. This is exactly what happened, but the decline in cases has been swifter than anyone predicted (more on this in the next section) causing me to over-predict cases by close to one million.
The deaths prediction was made with moderate certainty. For a few months the deaths heuristic (deaths lag cases by 21 days with a CFR of 1.7%) has worked extremely well and continues to do so.
At the end of February, I predict 28,710,000 confirmed cases and 516,000 confirmed deaths in the United States. The cases prediction is based on continued rapid declines in case loads. We would be at ~60,000 cases per day in this scenario. The deaths prediction is based on our deaths heuristic. The final 21 days of January had 3.9 million cases and at a CFR of 1.7%, that is ~67,000 deaths through just February 21st.
Why are cases declining so rapidly in the United States?

The seven-day average of cases in the United States peaked on January 12th at 256,517 cases per day. Today, the seven-day average is 120,476, or more than a 50% reduction in under a month. I’m not aware of anyone that predicted such a rapid decline, yet in hindsight, it makes perfect sense.
The more conspiracy-minded individuals on the internet have claimed that the Biden administration is manipulating the numbers, but this is nonsensical as 1) the states report their daily numbers and 2) both test positivity rates and hospitalization numbers (which would be very hard to fabricate) also suggest a rapidly declining caseload.
Even more suggestively, rapid declines like the one seen in the United States are occurring all across the Northern Hemisphere (below are the daily cases graph for the United Kingdom, Russia, Canada, and Japan).

Generally, the simplest explanation tends to be the correct one (Occam’s Razor). These rapid declines across the Northern Hemisphere should be a major clue. SARS-CoV-2, like all other endemic human coronaviruses and most respiratory viruses, exhibits large seasonal effects.
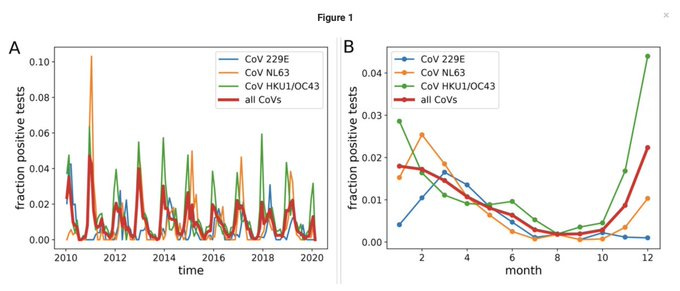
Below is a graph that I’ve included a few times. It shows the annual pattern of infection by endemic human coronaviruses. Look at CoV-HKU1 (green line) and CoV-NL63 (orange line). They display a rapid increase of infection starting in October, that peaks in December or January, and then rapidly declines throughout the spring. This appears to be exactly what SARS-CoV-2 is doing!
Updates on Vaccines and Variants
The news on vaccines remains incredible. This week, Johnson and Johnson filed for a Emergency Use Authorization with the FDA. The main advantage of their vaccine is that it only requires a single shot. All available evidence suggests that it will be approved on February 26th. Moreover, the Russian’s Phase III trial for the ‘Sputnik V’ vaccine was published in The Lancet this week.
The six vaccines with fully-published clinical trials are listed below (image credit to Dr. Monica Gandhi). All six exhibited a 100% protection from hospitalization and death (highlighted in yellow).

Vaccinations in the United States continue to scale and the seven-day average for daily vaccinations stands at an all-time high of 1.4 million. Bloomberg estimates that 9.5% of the American population has received a first dose and 2.7% have received a second dose.

68.3% of distributed vaccines have been administered. Administration numbers have now climbed to be roughly equal to distribution numbers, i.e. we are ‘getting shots in arms’ as fast as they can be manufactured. As we continue to scale vaccinations, it appears increasingly likely we will have a supply issue. Having Johnson and Johnson’s vaccine authorized should help relieve some of that issue. Meanwhile, Moderna is inquiring with the FDA about loading more doses per vial to speed distribution. AstraZeneca’s vaccine authorization continues to be delayed in the United States to some controversy.
The news on the variants remain mixed. It now appears that B.1.1.7 (the ‘United Kingdom’ variant) is the ‘triple-whammy,’ i.e. increased transmissibility, increased mortality, and some amount of immune escape.
Fortunately, while vaccines generally appear to show a minor reduction in effectiveness for mild disease (with perhaps an exception for AstraZeneca’s vaccine and B.1.351 (the ‘South Africa’ variant)), it appears they will continue to prevent hospitalizations or deaths.
Comments on Viral Evolution
As mentioned last week, these variants are subject to their own evolutionary pressures, just as the ‘original’ strain was. It now appears that B.1.1.7 is independently evolving the E484K mutation (one of the more concerning mutations). This is highly suggestive of convergent evolution, which in this case would itself be suggestive of a true increase in evolutionary fitness that all these variants have moved toward.
Viruses generally evolve quickly. But while these specific variants arose in less than a year, that does not necessarily mean newer variants will arrive on a annual basis.
Dr. Trevor Bedford did an excellent thread comparing SARS-CoV-2 evolution with influenza. The entire thread is excellent, but the important conclusion is highlighted below.

If you imagine the potential evolutionary ‘landscape’ as a terrain of peaks and valleys, the virus will start at some random location and work toward the nearest ‘fitness peak.’ But once at a peak, it is very hard to jump from one peak to the next one. In other words: large, meaningful evolutionary steps don’t happen very often.
Think of influenza. Influenza evolves rapidly enough that we do get new strains from year-to-year. But while these strains a different enough to merit a new vaccine, they also tend to be about as lethal as the year before (influenza has a CFR on the order of ~0.1%). It is only once-in-a-generation that an influenza virus takes a large evolution step and a hyper-severe influenza circulates.
Thank you for reading to The Counterpoint. Feel free to subscribe below at either the free or paid tier. I’m humbled by any and all support. If you think someone else would enjoy, please share the article. Leave any questions, comments, or suggestions in the comment section.