
SARS-CoV-2 Update For July 14th
SARS-CoV-2 Update For July 14th
BA.4 and BA.5 continue to run rampant in the United States. Cases and deaths have decoupled. Immunity from both vaccination and prior infection remains broadly robust. Vaccination uptake remains poor.

The Counterpoint is a free newsletter that uses both analytic and holistic thinking to examine the wider world. My goal is that you find it ‘worth reading’ rather than it necessarily ‘being right.’ Expect regular updates on the SARS-CoV-2 pandemic as well as essays on a variety of topics. I appreciate any and all sharing or subscriptions.
The seven-day average of daily cases in the United States is 126,552. This number has oscillated between 90,000 and 130,000 since May 16th, almost two full months. While this wave started with the rise of Omicron BA.2.12.1 in early April, it has been steadily displaced by Omicron BA.4 and BA.5. According to the CDC’s variant tracker, these two strains now represent 82.3% of current cases in the United States.
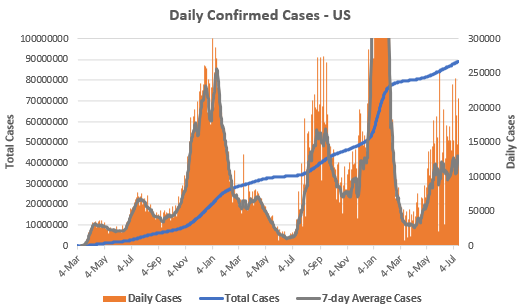
The true level of infection is certainly far higher. This has been an issue throughout the pandemic because of both asymptomatic illness and inadequate testing, but undercounts have been magnified during both Omicron waves by the availability of at-home rapid tests.
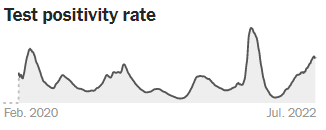
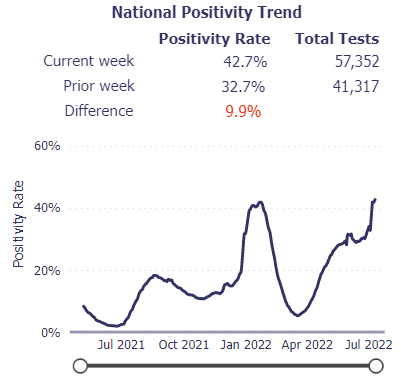
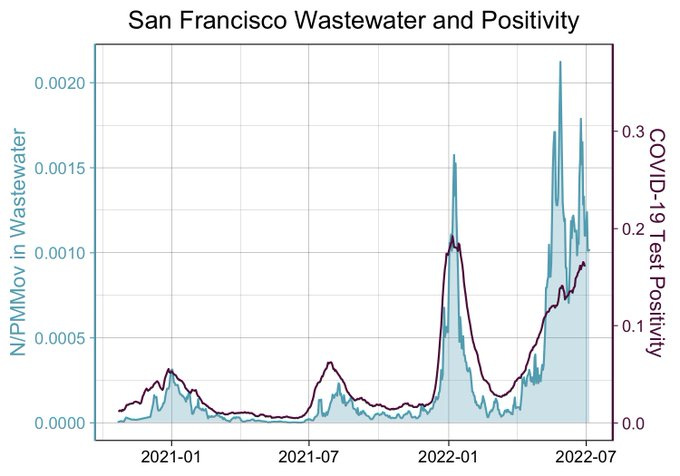
Multiple sources all suggest that current case loads are significantly higher. The New York Times (below, top), Walgreens (below, middle), and Johns Hopkins all report the second highest positivity rate ever. The CDC’s wastewater surveillance tracker shows that half of all sites are reporting a significant increase in the amount of viral RNA detected, with some sites even surpassing their Omicron BA.1 peak (e.g. San Francisco, below, bottom).
There is no such thing as a good wave of cases. We can all agree that the fewer cases the better. But thus the ‘paradox’ of the current wave. The true level of infection is far higher than current confirmed numbers. But the larger the current wave, the milder the average case must necessarily be.
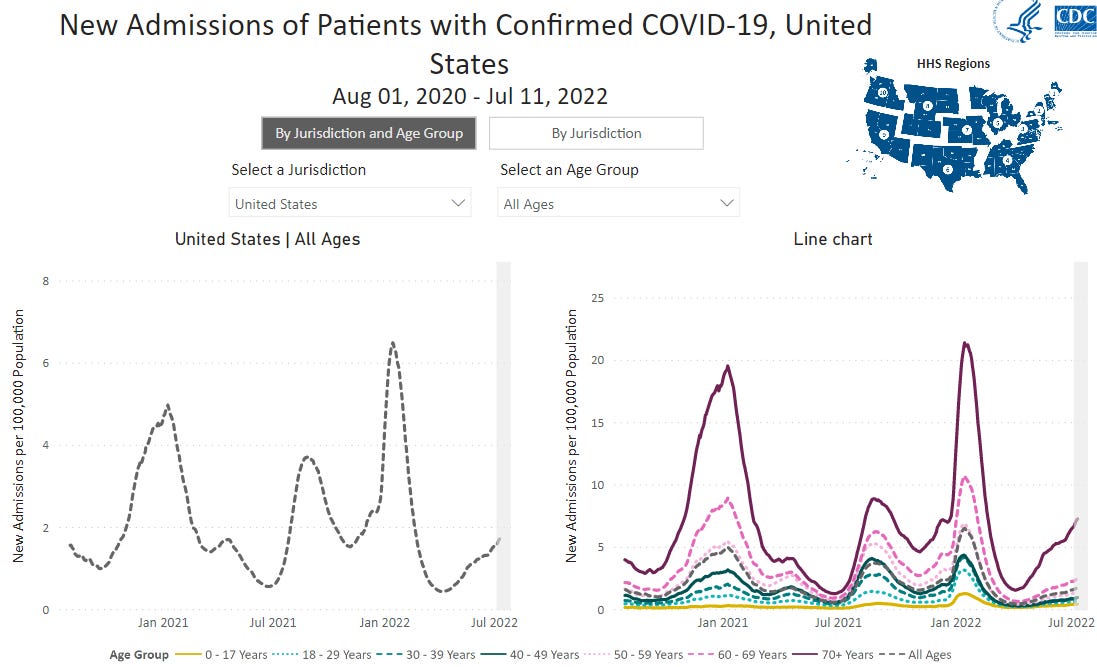
While the current wave has resulted in an increase in hospitalizations, the total rate remains below that of the prior four waves, including the Alpha wave in spring 2021 (below, left), when confirmed daily cases were last than half of current confirmed cases. Moreover, the current increase in hospitalizations is almost entirely people above the age of 70 (below, right). Age has always been and remains the number one risk factor for severe COVID-19.
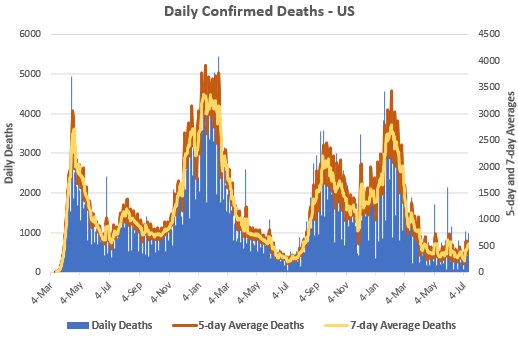
There has been an even larger divergence between cases and deaths. Despite what is possibly the second-largest wave of cases and a meaningful increase in hospitalizations, deaths remain near all-time lows. The seven-day average of daily cases is 531.
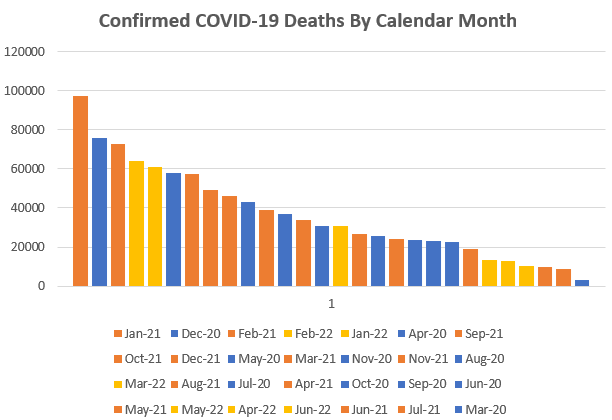
Along with June and July 2021, April, May, and June 2022 were the five months with the fewest confirmed COVID-19 deaths since March 2020. July 2022 is on pace for ~13,100 deaths.
Make no mistake: the current situation should be considered unacceptable. A wave of hospitalizations is yet another strain on our already-strained healthcare workers and hospital system. The current ‘lows’ in deaths annualize to over 132,000 annual deaths, which doesn’t even account for a highly-probably winter surge. Rampant CoV-2 is an active threat to senior citizens and the immunocompromised. Long COVID remains a risk to all.
But the divergence between cases and severe illness highlights the point that I’ve been trying to make over the last few updates: both vaccination and prior infection induce an immune response that remains robust against all current variants and strains.
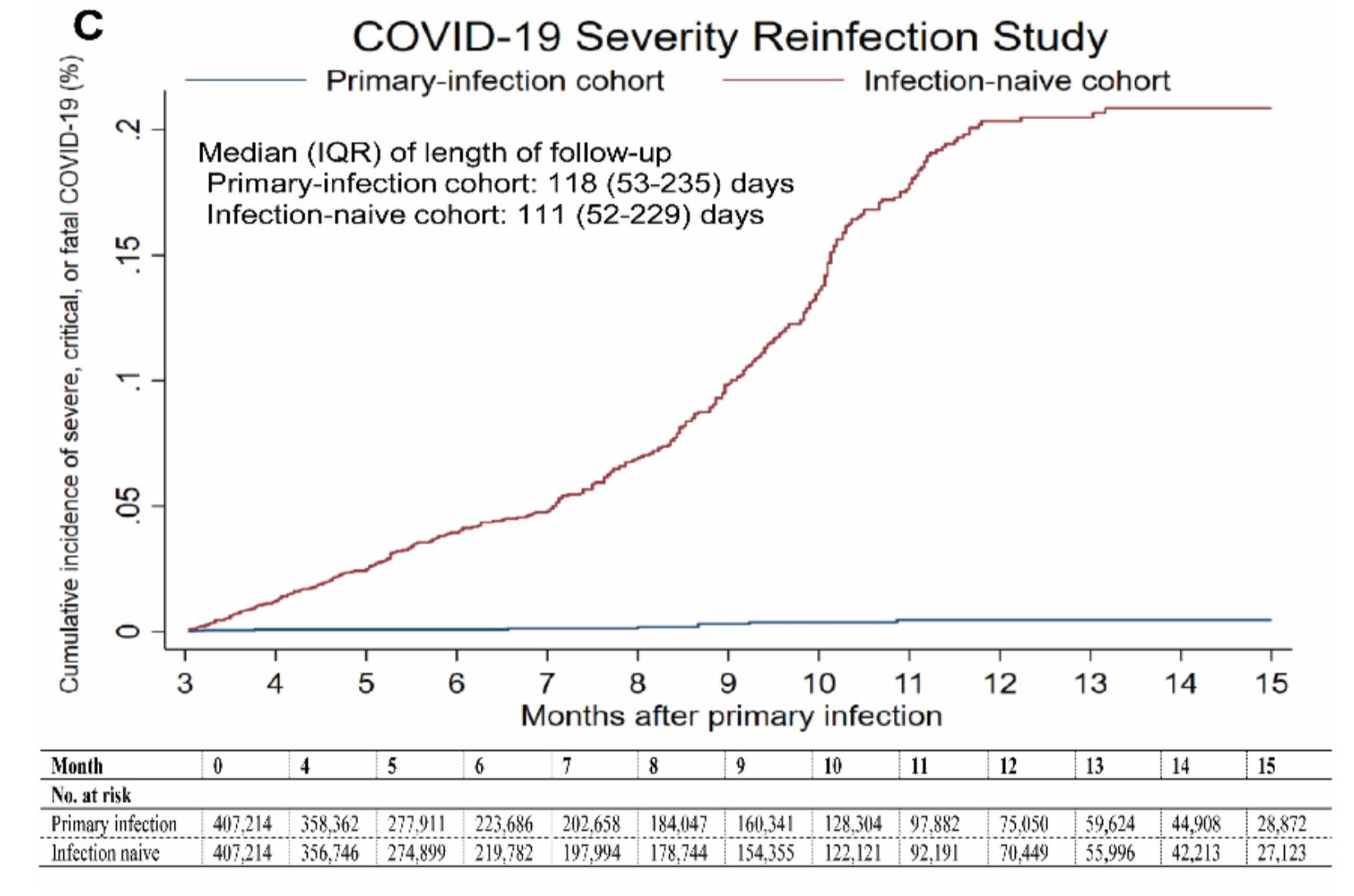
This was further emphasized by two pre-print studies published this month from the nation of Qatar in collaboration with Cornell. The first looked at pre-Omicron primary infection against pre-Omicron re-infection. The second looked at any primary infection against re-infection by specifically Omicron BA.4/BA.5.
The first study found an 85.5% effectiveness against any re-infection and a 97.3% effectiveness against severe, critical, or fatal re-infection (below).
The second study found that an Omicron primary infection provided a 76.1% effectiveness of against symptomatic BA.4/BA.5 reinfection and a 79.7% effectiveness against any BA.4/BA.5 reinfection.1
These studies do have an important caveat: Qatar is a very young country. The median age in each cohort in both studies was in the low 30s, while the median age in the United States is 38 and the median age in most other OECD nations is in the 40s. One’s individual risk may be very different from these population-level numbers.
But together, these studies continue to highlight that while reinfection is possible and BA.4/BA.5 do possess a meaningful amount of immune evasion, severe re-infections remain rare and at the population level, immunity remains robust against Omicron BA.4/BA.5.
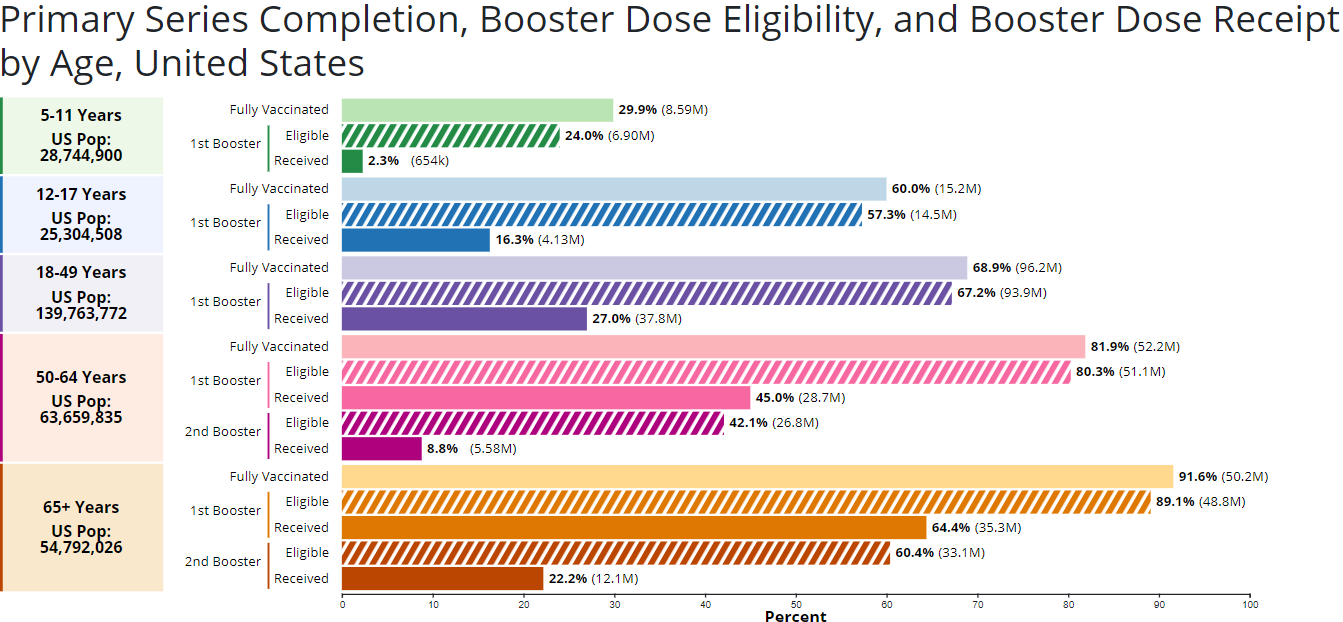
The elephant in the country remains that the United States remains incredibly under-vaccinated compared to other nations. There is no age group in the United States that has taken a third of available boosters. Only 2.3% of 5-11 year olds, 16.3% of 12-17 year olds, and 27.0% of 18-49 year olds have received their first booster. Only 8.8% of 50-64 year olds and 22.2% of senior citizens have received their second booster.
It cannot be emphasized enough that up-to-date vaccinations remains the single most important thing that any individual can do to reduce their risk from CoV-2 and COVID-19. Shared in the May 12th update were two studies that both suggested that second boosters provided an additional ~60% reduction in hospitalization compared to only one booster. Up-to-date vaccination means four shots (two primary and two boosters) if you are over 50 years old.
As mentioned previously, the current situation is unacceptable. But the current damage from the Omicron variants is primarily because the United States is under-vaccinated and poor access to the multiple classes of the therapeutics, not because Omicron BA.4/BA.5 are ‘super-variants that ignore immunity.’
Hospitalizations and deaths could be exponentially reduced by:
Increasing uptake of the current vaccines, especially second boosters for anyone over the age of 50.
Ventilation/sanitization upgrades for all public buildings.
Regular-updates to the vaccines so that they match current variants and strains. (Highly recommend Patrick Collison’s guest piece in Matt Yglesias’ Slow Boring)
A culture of voluntary mask-usage during a locality’s ‘cold & flu’ season or whenever cases are elevated.
Robust testing infrastructure so that clusters of cases can be quickly identified.
Increased manufacturing, distribution, and access to COVID-19 therapeutics such as Paxlovid, Evusheld, Bebtelovimab, and Fluvoxamine.
National paid sick leave.
It also found that a prior non-Omicron infection provided only a 15.1% effectiveness against symptomatic BA.4/BA.5 reinfection and a 28.3% effectiveness against any BA.4/BA.5 reinfection. If you have not being infected by an Omicron strain, I would take BA.4 and BA.5 much more seriously, especially if not up-to-date on vaccinations.