

SARS-CoV-2 Update for June 21st
A brief US update, a look at recent fatality rates in Portugal, comments on viral evolution, and the effect of time-of-day on vaccination

The Counterpoint is a free newsletter that uses both analytic and holistic thinking to examine the wider world. My goal is that you find it ‘worth reading’ rather than it necessarily ‘being right.’ Expect regular updates on the SARS-CoV-2 pandemic as well as essays on a variety of topics. I appreciate any and all sharing or subscriptions.
Brief United States Update
The seven-day average of daily cases in the United States is 104,353. This is just below the peak of the seventh wave at 121,973 on June 6th. According to the CDC’s variant tracker, Omicron BA.2.12.1 still dominates cases at 64.2%. But as discussed in June 9th’s update, BA.4 and BA.5 will likely displace BA.2.12.1 due their critical spike protein mutations which give them a meaningful amount of immune evasion. BA.4 and BA.5 are estimated to be causing 8.3% and 13.3% of current cases, respectively.
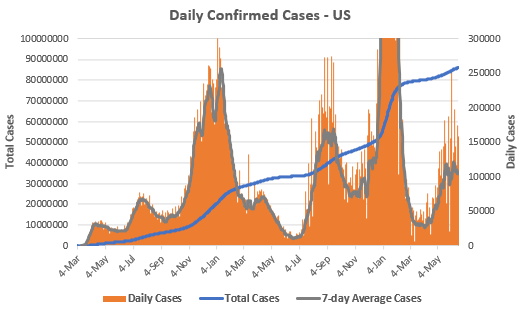
Deaths in the United States have plateaued near all-time lows. In the last week, 2,139 Americans have died, or ~306 per day. There have been 6,453 confirmed COVID-19 deaths through June 19th. At this rate, June will be the least deadly month of the pandemic, except for June and July 2021, right before the Delta wave. However, this rate annualized would still mean over 100,000 annual COVID-19 deaths in the United States.

Fatality Rates in Portugal
In previous updates, I’ve tried to reinforce that while the new Omicron strains are causing a wave of cases, these cases are leading to fewer deaths than any previous wave, despite the strains being more virulent. This is because immunity from both vaccination and/or infection remains robust.
But I’ve also emphasized that this is at the population level. One’s individual risk can vary drastically based on risk factors. Age has always been and remains the number one risk factor for severe COVID-19.
A good illustration of this is Portugal, which is a highly-vaccinated nation that experienced a large BA.1 wave, a moderate BA.2 wave, and now a large BA.5 wave.
The National Health Service of Portugal released a report (warning: Portuguese) on their current COVID-19 situation. Below is a graph from the report illustrating the fatality rates since May 2022 by decade of age and vaccination status.
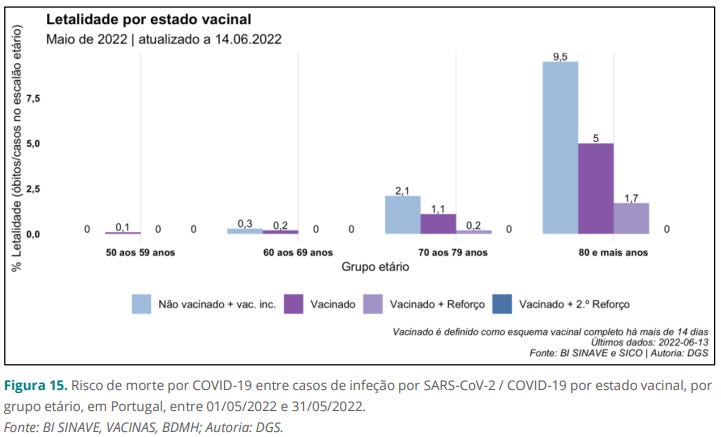
Unvaccinated (não vacinado) 80+ year olds have a fatality rate of 9.5%. This falls to 5% with two vaccinations (vacinado) and 1.7% with a booster (vacinado + reforco). These numbers decrease in a predictable pattern by age and vaccination status until the 50-59 age group, where deaths are minimal, even in the unvaccinated group.
(Keep in mind that after three large Omicron waves, it is likely that the vast majority of people in Portugal have immunity-via-infection. “Unvaccinated” should not be interpreted as “immune-naive.”)
While this emphasizes the continued effectiveness of vaccines, it also illustrates that they cannot be the only layer of protection for vulnerable populations. COVID-19 remains a serious disease in the elderly and immunocompromised. If you are at risk for severe COVID-19, focus on ventilation, wear high-quality masks, schedule your second booster, and ask your physician about prophylactic monoclonal antibodies.
Where Are All These Variants/Strains Coming From?
Below is a phylogenetic map that illustrates the major lineages of SARS-CoV-2 as well as their genetic distance (i.e. the more genetically distinct one strain is from another, the further they will be away from each other in the map).
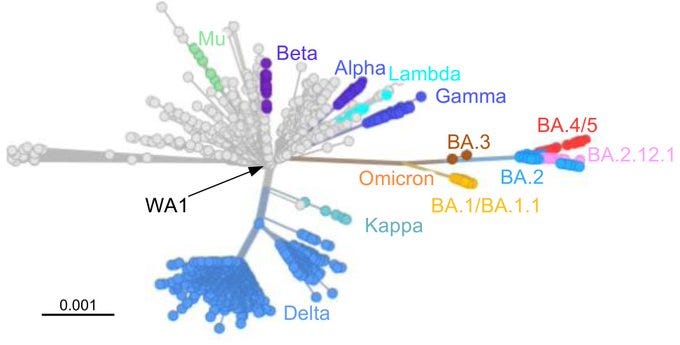
Notice that except for the new Omicron strains, all the major variants evolved from the wild-type (WA1) lineage, not from each other. This suggests that each major variant evolved independently, likely from a chronic infection in an immunocompromised host. The chronic infection allows the virus to ‘train’ against the human immune system and accumulate beneficial mutations.
The evidence supports this as well. For a journalistic article, read here. For the science, read this case report in New England Journal of Medicine, this correspondence in The Lancet, this pre-print on BioRxiv, or this letter to the editor in New England Journal of Medicine.
Again, this illustrates the multiple layers of protection that we need to emphasize when interacting with at-risk populations. In addition to protecting them from disease, it also potentially protects everyone from the rise of a new variant.
In the long-term, chronic infections in the immunocompromised are unlikely to be the only source of SARS-CoV-2 evolution. CoV-2 has shown a remarkable capacity for infecting other species (for example: minks and deer). These animal reservoirs can and will change CoV-2 in unpredictable ways. Moreover, co-infections of CoV-2 and other viruses present a risk because viruses can swap genetic material with each other, again opening the risk of CoV-2 changing in unpredictable ways.
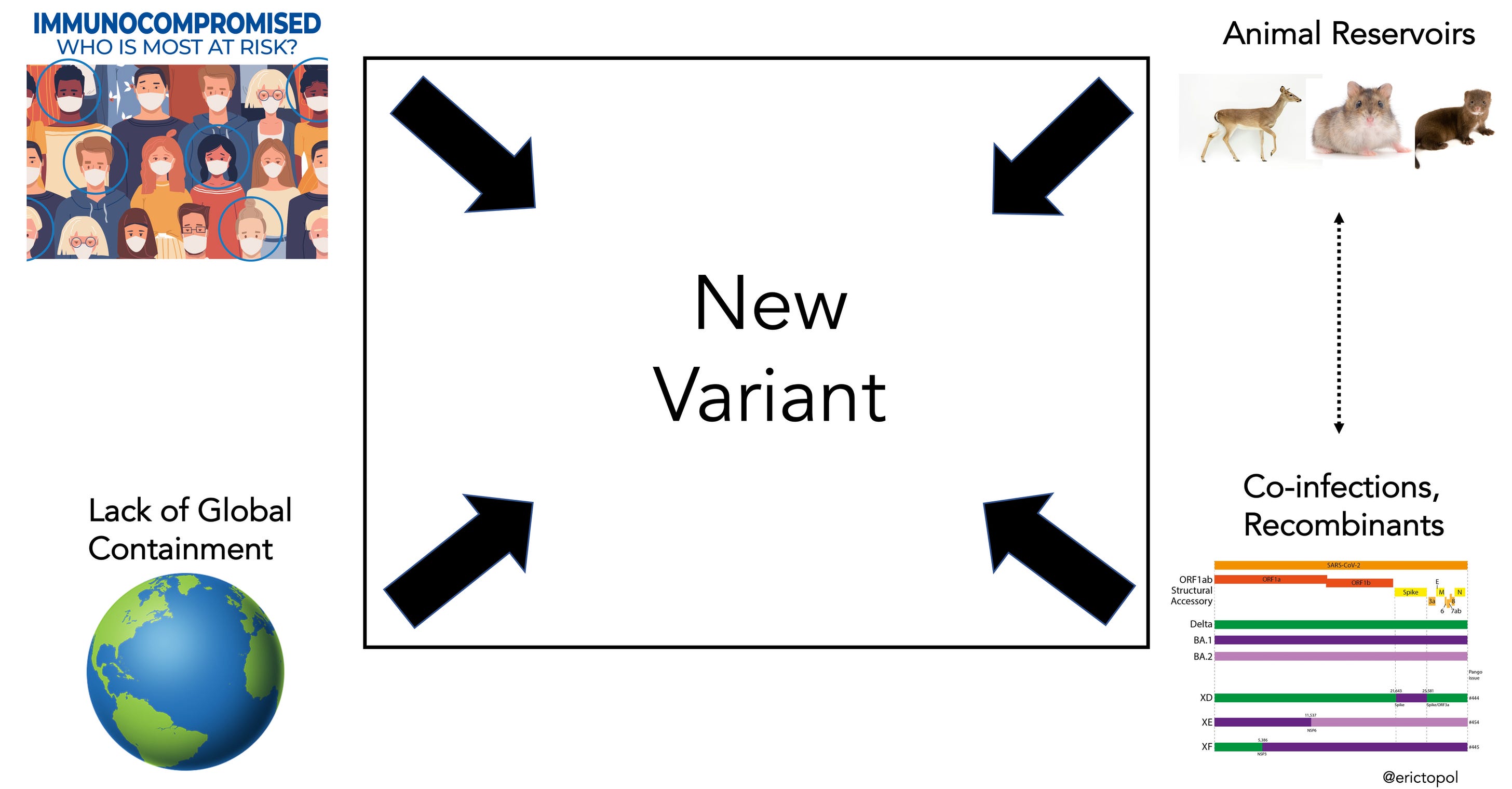
The crux of the issue is the lack of global containment. A “Zero COVID” strategy is no longer possible and destined to fail. CoV-2 is an endemic virus in the human population and will be with us for the rest of our lives.
But this doesn’t mean we can’t do anything. This only further emphasizes the importance of viral surveillance and maintaining testing capacity, so that outbreaks can be quickly identified, viral evolution monitored so that vaccines can be updated, and a nationwide effort to upgrade ventilation systems so that the spread of all airborne viruses can be slowed.
Vaccines and Circadian Rhythms
Circadian rhythms are physical, mental, and behavioral changes that follow a 24-hour cycle. The immune system is subject to these rhythms and the evidence has accumulated that they can influence how one responds to vaccines.
Scheduling your next vaccination for the morning could increase its effectiveness.
Two studies from last fall (Time of day influences immune response to an inactivated vaccine against SARS-CoV-2 and Timing vaccination against SARS-CoV-2) both found stronger immune responses were elicited with morning vaccination of COVID-19 vaccines.
Apparently, this has been found with other vaccines, including the BCG and influenza vaccines. See below.
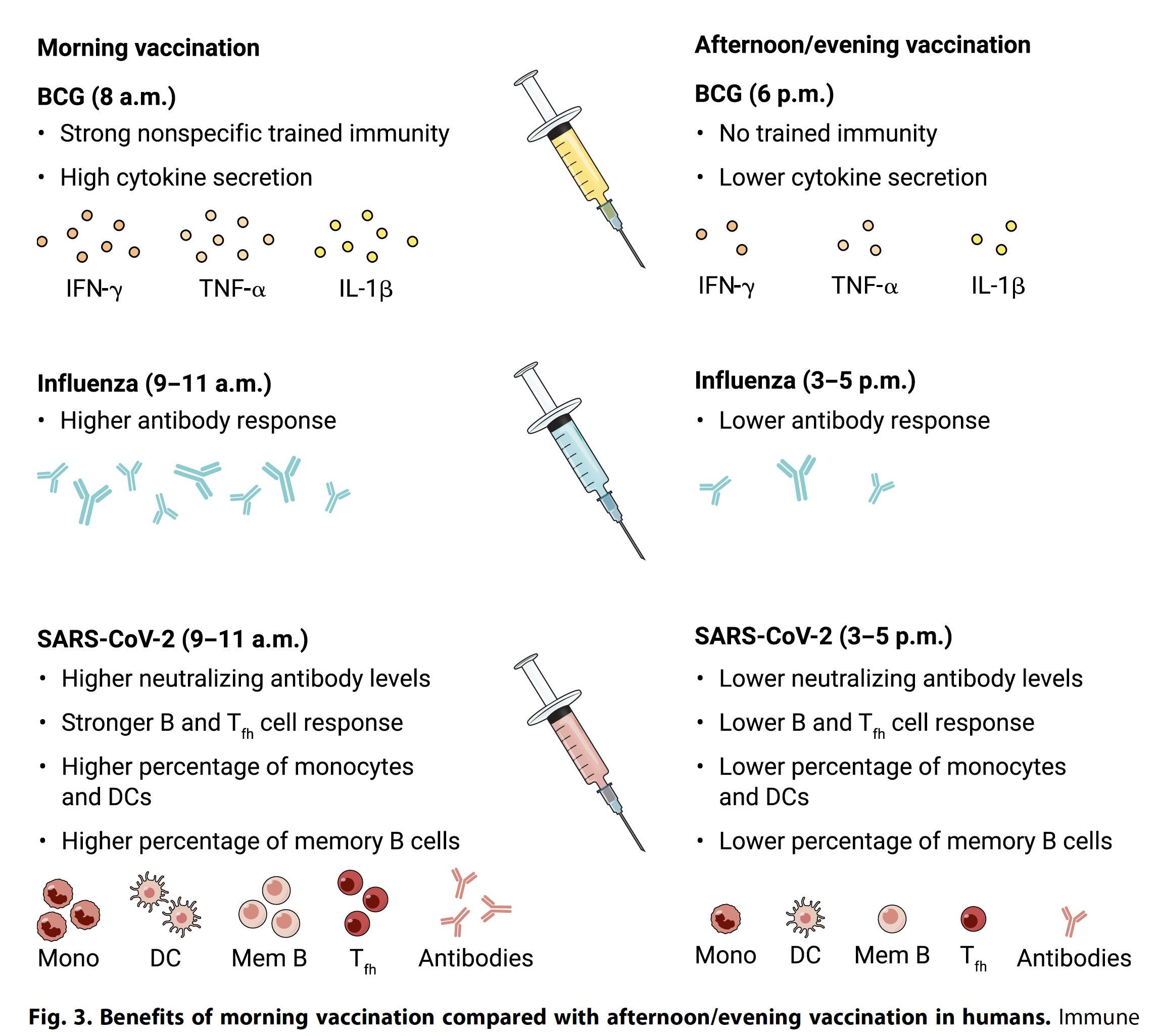
I wasn’t aware of this but will now be scheduling all vaccines for myself and my family in the morning.