

SARS-CoV-2 Update for May 24th
The latest US numbers, and updates on vaccinations, breakthrough infections, variants, and the CDC's updated guidelines.

The Counterpoint is a free newsletter that uses both analytic and holistic thinking to examine the wider world. My goal is that you find it ‘worth reading’ rather than it necessarily ‘being right.’ Expect regular updates on the SARS-CoV-2 pandemic as well as essays on a variety of topics. I appreciate any and all sharing or subscriptions.
Slowly but surely, the SARS-CoV-2 pandemic is coming to an end within the United States and other highly vaccinated countries. Globally, cases are below-peak yet remain elevated at ~586,000 confirmed cases per day. These cases are concentrated in unvaccinated nations, including many ‘pandemic overachievers,’ such as Taiwan, Uruguay, and Thailand. The story of the last five months is clear, undeniable, indisputable, and irrefutable: the vaccines are both safe and highly effective.
There have been 33,118,927 confirmed cases of COVID-19 in the United States. After nearly six consecutive weeks of declines, the seven-day average of daily cases is 25,344, the lowest since June 18th, 2020.

There have been 589,920 confirmed deaths from COVID-19 in the United States. The seven-day average of daily deaths is 563, the lowest since April 1st, 2020.

Throughout the pandemic, we’ve covered how cases and deaths are correlated, with deaths lagging cases by approximately three weeks. Yet the fourth wave of cases in spring 2021 did not lead to any noticeable increase in deaths. Disregard the data dump on April 8th, and deaths have been on a steady decline since mid-February. When vaccinations are concentrated on those at-most-risk, as they were in the first months of 2021, the correlation between cases and deaths breaks.
Despite declines in daily vaccinations, the United States continues to be one of the most highly-vaccinated nations. 285,720,586 doses have been administered in the US, with 49.2% and 39.2% of the population being partially and fully vaccinated, respectively. The seven-day average of daily vaccinations is 1,739,340.

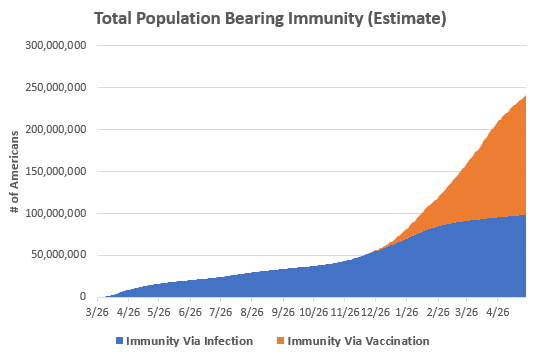
Combine the above confirmed cases and daily vaccinations graphs and it should be clear why cases are declining so rapidly: the majority of the population carries immunity to SARS-CoV-2, whether by infection or vaccination. Our simple model suggests that ~241 million Americans bear immunity. Of course, there is some overlap between these groups so the true number is smaller, but the point remains that we are nearing herd immunity. This threshold would be 218 million Americans (66.6%) or 264 million Americans (80.0%) assuming R0s of 3.0 and 5.0, respectively.
But herd immunity isn’t the end. Cases (and deaths) do not magically stop once that threshold is hit. Herd immunity is merely the point at which all case clusters will burn out on their own, even with no public health measures. There will still be carriers of the virus within the population and all unvaccinated people will continue to be at-risk. Should large numbers of unvaccinated people congregate for extended periods in poorly-ventilated areas, local ‘waves’ will still be possible.
Summer seasonality effects combined with continued vaccinations should suppress cases to nearly zero throughout the summer and early fall, but depending on how vaccination campaigns fare in coming months, there may be non-negligible outbreaks of SARS-CoV-2 throughout winter 2021/2022.
Two weeks ago, news broke that nine vaccinated New York Yankees tested positive for SARS-CoV-2. While it is common knowledge that the vaccines are not 100.0% effective at preventing infection, such a large cluster within a single, vaccinated group caused a negative reaction in many people. Yet this story is one of our strongest, real-world examples that the vaccines are highly effective.
Yes, this was a cluster of infections in vaccinated individuals, but let’s think about the New York Yankees. Being a professional sports franchise they are tested regularly, like “everyone in the Yankees’ traveling party of 50 to 60 people is being tested three times a day using polymerase chain reaction, saliva, and rapid tests” regularly. With that level of scrutiny, the organization is going to detect every single case, whether symptomatic or not. In fact, only two people in the cluster was symptomatic, and they both had mild symptoms that went away after just a few days. The rest were completely asymptomatic and probably never would’ve known that they were infected had they not been tested so frequently.
But Patrick, we’ve known about asymptomatic cases for over a year now. This is still infections in fully-vaccinated people! True, I’m not denying the infections. But let’s think deeper about the Yankees.
One of the most famous case reports of the entire pandemic is the Skagit County choir practice. In March 2020, a single 3-hour choir practice of 61 people led to 32 confirmed and 20 probable COVID-19 cases (for an attack rate of 53.3% to 86.7%). Three patients were hospitalized and two died!
Meanwhile, the Yankees are an organization of dozens of players, coaches, and trainers that regularly spend extended periods of time together. Moreover, some of that time involves heavy breathing. If a single afternoon of choir practice produces an attack rate of 53.3% to 86.7%, an outbreak within the Yankees should’ve produced similar (if not worse) results. If the Yankees traveling party is 50-60 people, there should’ve been anywhere from 27 (using 50 people, 53.3% AR) to 52 cases (using 60 people, 86.7% AR).
Let’s be generous and use the smaller case number. If we expect 27 cases within a given context, but only nine cases occurred, then that is a 66.7% reduction in cases.
All the New York Yankees were vaccinated with Johnson & Johnson vaccine. The CDC reports the Johnson & Johnson vaccine as 66.3% effective.
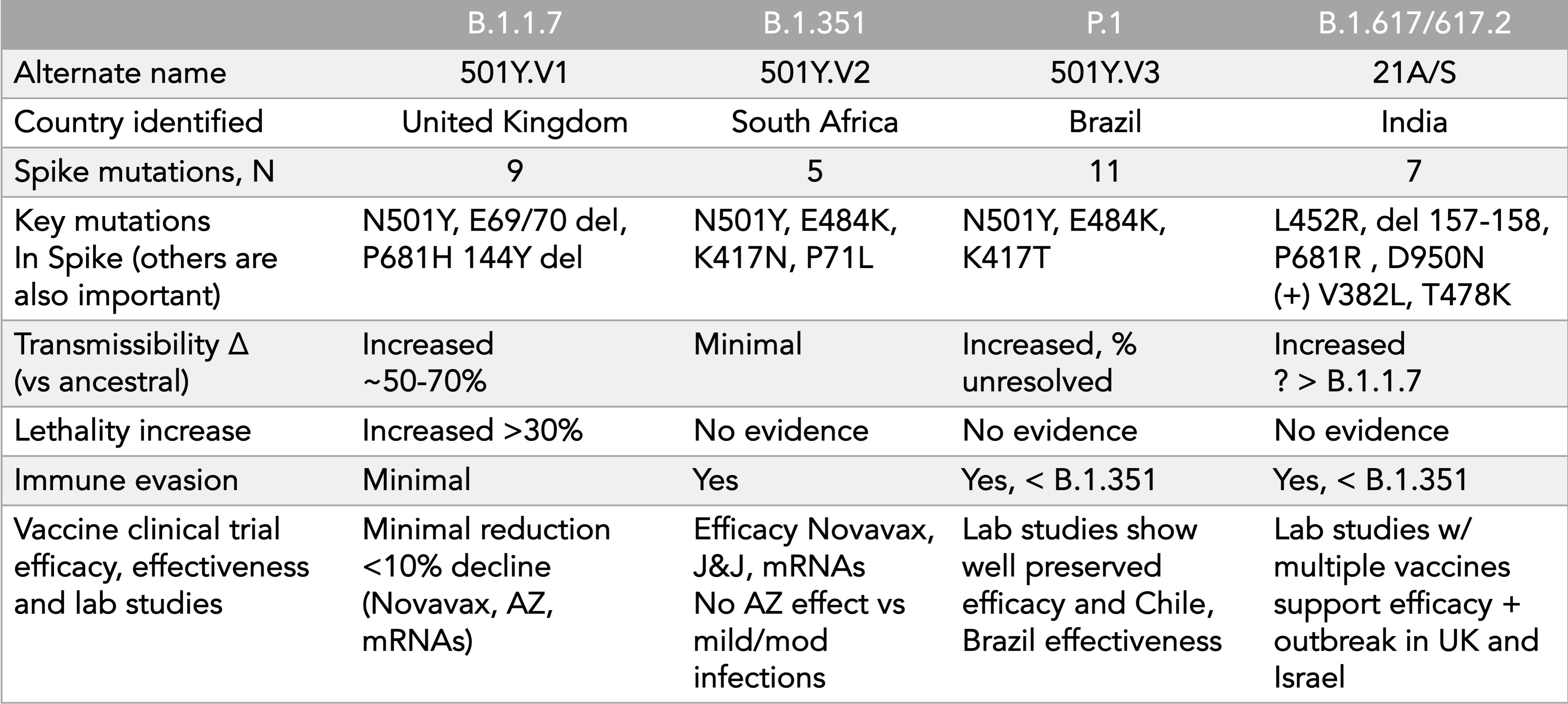
There is a new variant-of-concern: B.1.617, first identified in India. This is now the fourth variant in the highest risk category. All four are being monitored extensively and all current evidence suggest the vaccines remain effective against each of the four. The below chart summarizes these four variants, courtesy of Dr. Eric Topol:
The concern with the new B.1.617 was not only the large and devastating wave of cases in India, but more importantly the fact that B.1.617 seems to be outcompeting the already-more-infectious B.1.1.7 ‘United Kingdom’ variant. Below is a graph shared by Dr. Trevor Bedford showing the frequencies of the variants over time in India (the whole thread is worth reading). A similar increase in frequency has been observed in the United Kingdom. Dr. Bedford’s conclusion: “If faster growth than B.1.1.7 in India and in the UK is conclusive, it would suggest that this lineage will spread widely.”


Fortunately, the United Kingdom has published its preliminary studies against this variant and the vaccines remain highly effective (~87%) against B.1.167, but only after two doses. For unknown reasons, this strain exhibits marked reduction in vaccine effectiveness (~34%) after only one dose. All the more reason to schedule your second shot.
On May 13th, the CDC abruptly removed its mask and distancing guidelines for the fully vaccinated. While this was a decision that I wouldn’t have made and don’t agree with, I don’t think it was a bad decision. Let me explain:
I wouldn’t have made the decision because the shear reality of the situation is that nearly 600 Americans are dying per day from a preventable disease, masks help prevent the spread of that disease, and there is zero cost or risk in wearing a mask. With millions of Americans being vaccinated per day and seasonality effects steadily increasing, combining these effects with continued public health measures would’ve been the perfect opportunity to truly crush this virus into negligibility.
But I also don’t think it was a bad decision because, to be glib, the masks have to come off sometime (though please put them back on, voluntarily, next cold and flu season).
Phrased more seriously, while the CDC’s decision was riskier than my own personal calculus, I don’t think it was risky, per se. As we saw above, immunity is broad-based and case counts have been declining for multiple, consecutive weeks. Moreover, using a ‘masks off’ carrot as motivation for the unvaccinated is not a terrible idea (Personally, I favor things like Ohio’s vaccine lottery or Alabama’s letting-you-drive-on-Talladega-Speedway). Finally, at this point in the pandemic, people’s individual choices are more likely a function of their individual risk tolerance than of broad public policy. Derek Thompson wrote about that phenomenon within the microcosm of Texas.
To the latter point, I’m continuing to wear a mask in public (my personal ‘mask off’ date is June 15, if you must know). But if you are vaccinated, I don’t begrudge you if you don’t wear one.
And one final point: please schedule your vaccination. Also, encourage someone else to schedule theirs, or even better, help them schedule it. Vaccinations save lives.