The Delta Variant Explained In Four Simple Graphs

The Counterpoint is a free newsletter that uses both analytic and holistic thinking to examine the wider world. My goal is that you find it ‘worth reading’ rather than it necessarily ‘being right.’ Expect regular updates on the SARS-CoV-2 pandemic as well as essays on a variety of topics. I appreciate any and all sharing or subscriptions.
Since its emergence, SARS-CoV-2 has been subjected to evolutionary pressures. With the rise of low-cost, high fidelity genomic sequencing, the scientific community has been able to track SARS-CoV-2 more than any previous disease. Find the full ‘family tree,’ containing thousands and thousands of variants, here via NextStrain.
Most of these mutations do not affect viral fitness, i.e. its ability to transmit, infect and/or cause disease. However, a more fit virus did (and will) evolve, and that fitter virus did (and will) outcompete any less fit strains.
The first occurrence was very early in the pandemic with the D614G mutation, which went from ~0% of sequences in March 2020 to ~75% of sequences by June 2020. By fall 2020, newer variants had emerged. In September, the Alpha variant (or B.1.1.7) in the United Kingdom and in October, the Beta variant (or B.1.351) in South Africa. The Alpha variant was especially concerning because preliminary evidence, which has now been confirmed, suggested it is 40-80% more transmissible than D614G.
During the spring 2021 surge in India, the strongest yet variant evolved. Known as the Delta variant (or B.1.167.2), it is rapidly displacing previous variants, suggesting it is extremely transmissible and it appears to have the ability to escape antibodies in partially-vaccinated individuals.
While the science behind the Delta variant is interesting, it isn’t what the average person needs to know. Both scientific experts and general media can be poor communicators, getting bogged down by technical details or hyping up doomsday interpretations. Everything you need to know about the Delta variant can be learned from the following four images.
Both the United Kingdom and South Africa were places where variants-of-concern were first identified. Despite the prevalence of highly-infectious variants within those countries, the Delta variant has rapidly displaced them; it is a supermajority of sequences in both countries.

Despite both countries being hard hit by previous waves, the hyper-infectious Delta variant is causing a new wave of cases in both countries.

There are differences between the United Kingdom and South Africa, e.g. access to healthcare, quality of healthcare, median age of the population, Northern vs Southern Hemisphere, etc. But the most important difference with respect to SARS-CoV-2 is that the United Kingdom is highly vaccinated, with 67.5% of the population having at least one dose of vaccine, while that number is only 6.3% in South Africa.
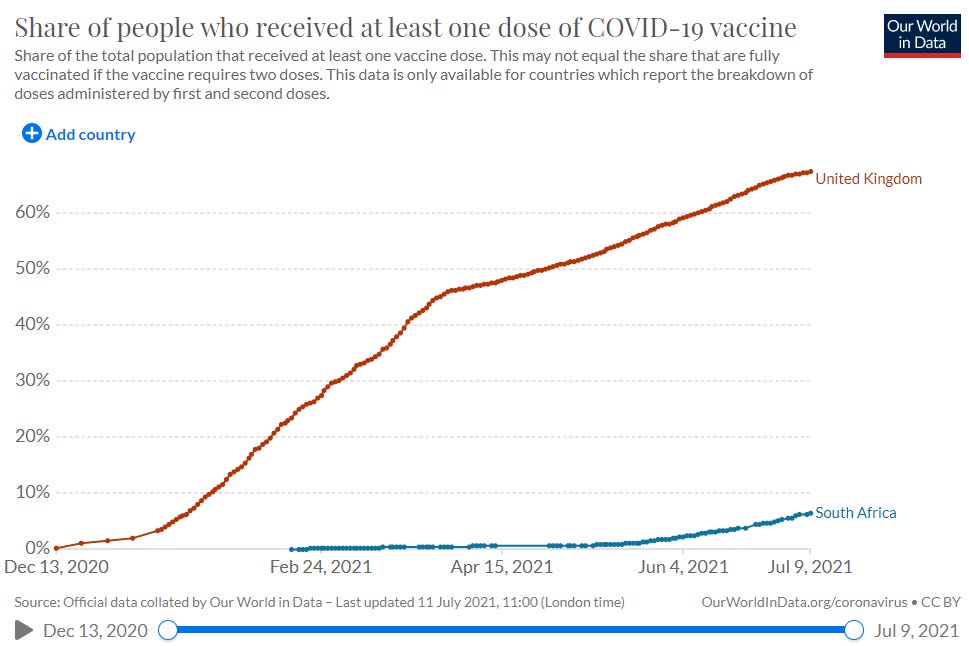
Because of this, despite similar increases in the Delta variant leading to similar surges in cases, only one country is having a surge in deaths.

The complete, two-dose vaccination doesn’t always protect from contracting SARS-CoV-2. But the evidence is overwhelming that it does protect from serious disease and death.
One final graphic: The Delta variant is now the dominant strain of SARS-CoV-2 within the United States. It is causing a surge of cases in many states and some are having a surge in hospitalizations. All share one common characteristic: each ranks in the bottom half of total vaccinations.
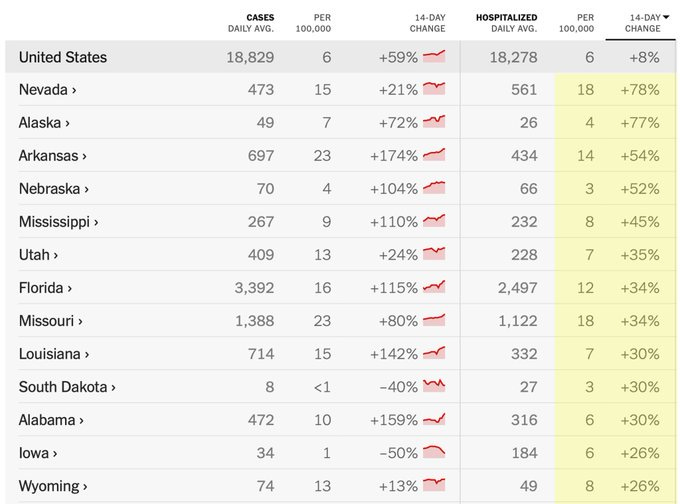
If you know someone that is unvaccinated, please encourage them to schedule an appointment.