

The Delta Wave: the Good, the Bad, the Ugly Pt. 2
Cases, hospitalizations, and deaths all continue to rise, but there are signs of peaking. Vaccines remain highly effective. The situation is likely to remain severe throughout this fall and winter.

The Counterpoint is a free newsletter that uses both analytic and holistic thinking to examine the wider world. My goal is that you find it ‘worth reading’ rather than it necessarily ‘being right.’ Expect regular updates on the SARS-CoV-2 pandemic as well as essays on a variety of topics. I appreciate any and all sharing or subscriptions.
The Delta wave continues; the seven-day average of daily confirmed cases is 170,528 (below). In retrospect, this was the only outcome. Returning-to-normal, reducing or removing public health measures, and decreasing total testing volume, despite the evolution of a hyper-infectious variant in spring 2021, when the population was mostly unvaccinated (only 46.7% of Americans were fully vaccinated on July 1st) all added up to our second-largest (and growing) wave of cases.

Fortunately, there are signs of cases peaking; the ‘leading-edge’ states such as Arkansas, Missouri, and Louisiana are seeing declines in daily cases. But to be clear, the majority of states are continuing to see increases in cases, and we aren’t even at the start of ‘cold & flu’ season.
The current situation is complex and defies easy explanation. It is neither doomsday nor back-to-normal. Some good, bad, and ugly caveats are explored below.
The Good
All authorized vaccines continue to provide robust protection from serious disease and death due to COVID-19. This point cannot be reiterated enough.
In a preprint published this week, researchers analyzed outcomes in Bahrain, a country where numerous types of vaccines are approved. Every vaccine significantly reduced hospitalizations, in both those older and younger than 50 years old.
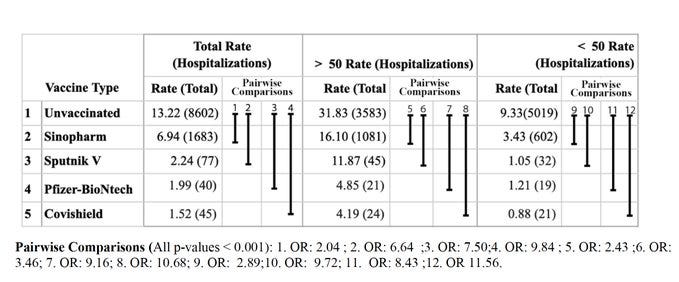
Now, Bahrain isn’t the United States, and most of these vaccines aren’t authorized in the US. But all United States-specific data supports the same conclusion: the vaccines continue to provide robust protection from hospitalization and death.
Published this week in Lancet, was a retrospective cohort study using Kaiser Permanente (the largest integrated healthcare system in the US). While they found that the effectiveness against infection of the Pfizer vaccine decreased over time (from 88% to 47%), vaccinated individuals continued to have a 89-92% reduced risk of hospitalization, regardless of age (below, bottom).

Even setting aside these studies and focusing solely on real world data, the relationship is clear. 18 of the 20 states with the highest rates of hospitalization have below-average vaccination rates. Credit to Charlie Bilello.

The Bad
SARS-CoV-2 is an endemic human virus. Each and every one of us will be infected at one point. Of course, there are many endemic disease (influenza, etc.).
The issue is that the SARS-CoV-2 Delta variant is both hyper-infectious and more likely to cause severe disease. Moreover, whatever one’s individual risk of severe disease, that risk is *in addition* to other disease.
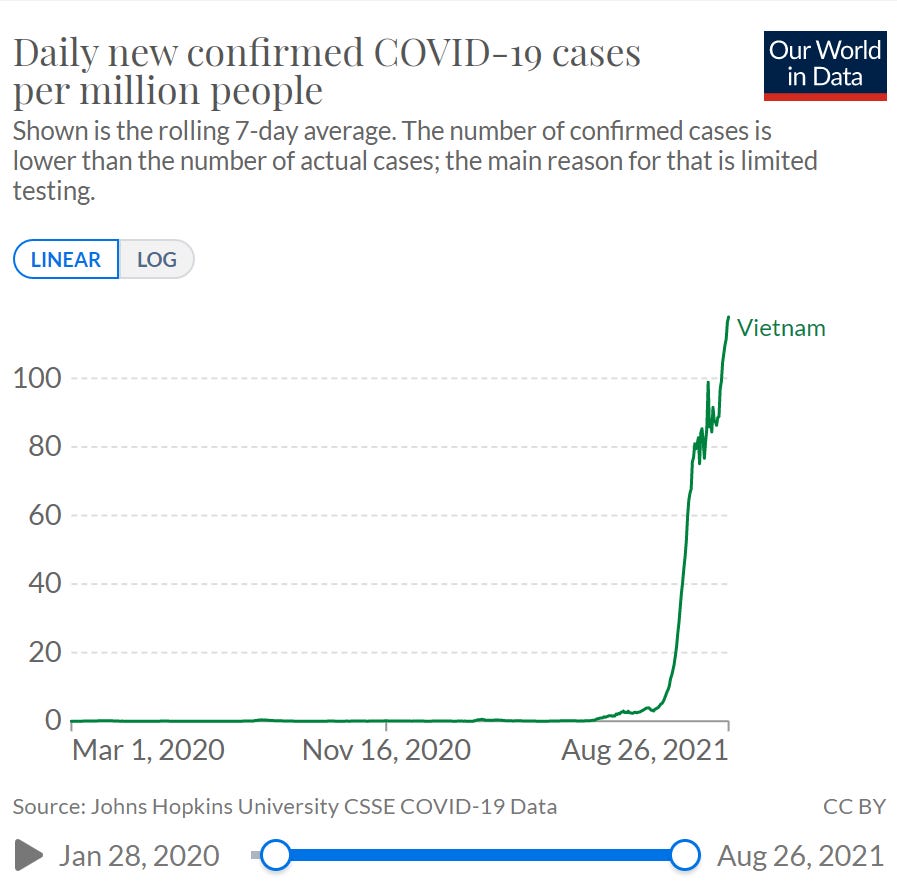
It’s been known for some time that Delta is more transmissible than even-previously-more-transmissible variants. To contextualize just infectious Delta is, let’s look at Vietnam, one of the best performing countries against SARS-CoV-2. They are currently going through their largest wave yet and their government instituted stay-at-home orders. Despite being perhaps the most ‘locked down’ nation in the world right now (below, top), their Delta wave shows no signs of slowing (below, bottom). A similar situation is occurring in New Zealand, another A+ performer. They issued a stay-at-home order after detecting a single case. Their cases continue to grow exponentially. Delta is simply too infectious.

Moreover, the evidence continues to suggest that it is also more likely to cause severe disease than previous variants. Published yesterday in Lancet Infectious Diseases was the highest quality study on this yet. To quote the authors: “This large national study found a higher hospital admission or emergency care attendance risk for patients with COVID-19 infected with the delta variant compared with the alpha variant.”
This goes a long way in explaining the current hospitalization graph within the United States (below). 95,323 Americans are in the hospital because of COVID-19. 24,872 are in the ICU.

Of course, one’s vaccination status will heavily influence the outcome of SARS-CoV-2 infection. The majority of the above hospitalizations are the unvaccinated. But other factors are also at play. Just as numerous factors influence the severity of car accidents (speed of the vehicles, inclement weather, seatbelts, etc.) there are numerous factors that influence the severity of SARS-CoV-2 infection (vaccination status, age, sex, co-morbidity status, etc.).
The Israeli health ministry released data putting this in perspective. A *fully-vaccinated* 70-year-old has the same risk of developing severe disease from SARS-CoV-2 infection as an *unvaccinated* 40-year-old (below).
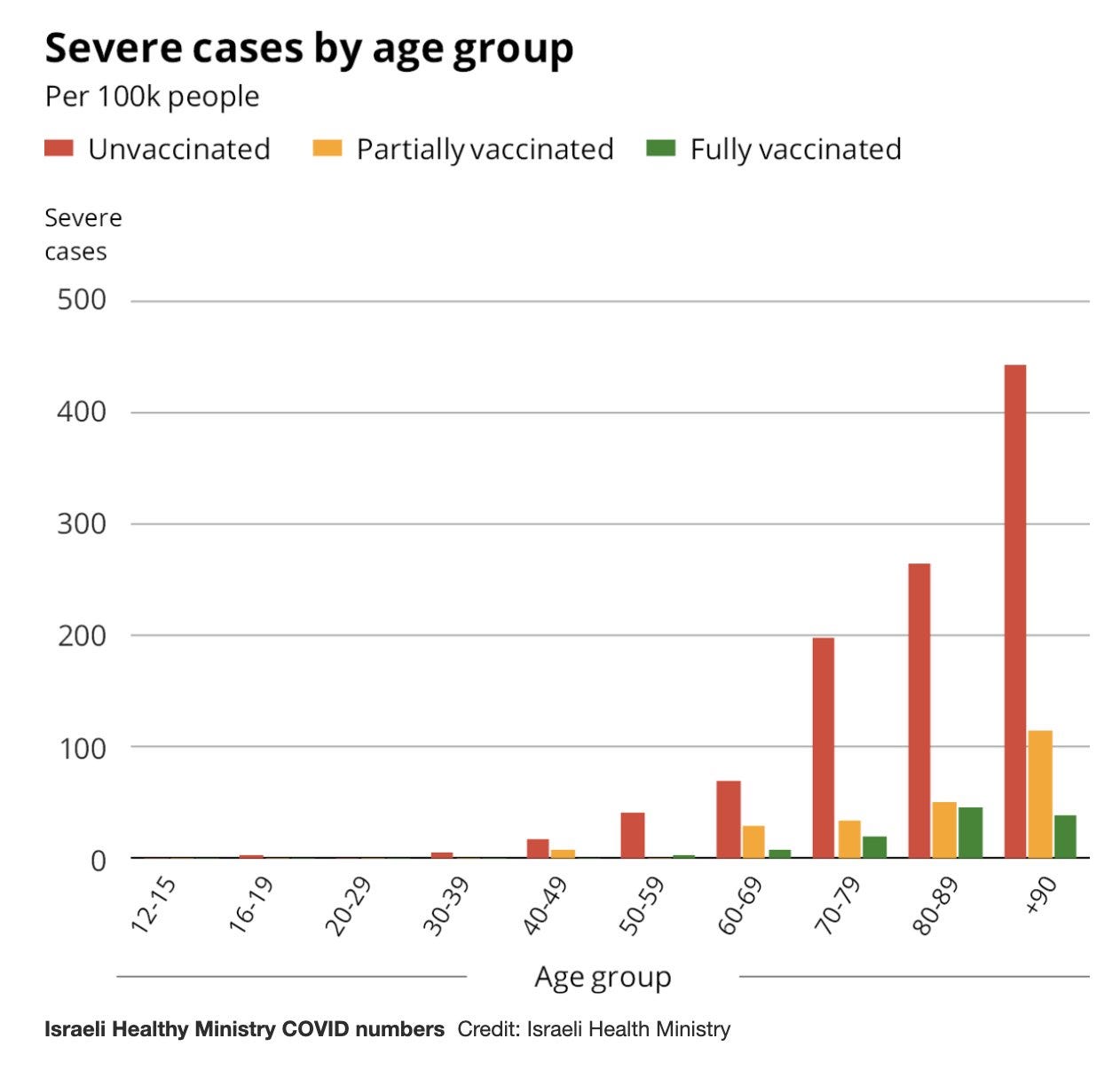
Now, unvaccinated 40-year-olds aren’t the cohort that comes to mind when one thinks of COVID-19 risk. Yet, 20,523 of them have died since the beginning of the pandemic.
To be clear, most of these occurred prior to the vaccines and the vaccines will certain drastically reduce the annual COVID death toll. But let’s assume we’re at 700,000 total deaths by Dec 31, 2021 (we’re on pace to be above that number). This would mean 350,000 deaths per year (in fact, a little more, since COVID deaths didn’t start until March 2020). If one assumes the vaccines reduce that by 90%, that would still mean 35,000 annual COVID deaths annually, each and every year, putting it just outside of the top ten annual causes of death.

SARS-CoV-2 and COVID-19 are likely with us forever. The annual ‘cold and flu’ season will now be the annual ‘cold, flu, and COVID season.’ Whatever one judges the risk of COVID-19 to be, that risk is *in addition* to all other disease risk.
The Ugly
It’s likely to be a very rough school year. It should be clear what happens when unvaccinated individuals congregate in poorly-ventilated, indoor rooms for extended periods of time: the Delta variant exploits it. Children are unvaccinated; schools are poorly ventilated.
Education is extraordinarily important for children. And as the previous section made clear, SARS-CoV-2 is endemic. We have to learn to live with the virus. But sending millions of unvaccinated children without public health measures into old school buildings without ventilation is beyond absurd. The South tried this and now the pediatric hospitalization rate is HHS Region 4 (the Southeast) is as high as the hospitalization rate for 40-year-olds in HHS Region 1 (the Northeast).


In-person education is extremely important. There are two ways we could reduce the problem. Either vaccinate children or practice strict public health measures (or even better, both).
Israel has started vaccinating children ages 5-11 that are at risk of disease (with 1/3rd the dose of the normal shot, unclear how that was determined). How the FDA looks at the pediatric hospitalization rate in the Southeast and doesn’t immediately conclude that vaccine *authorization* for children is *less risky* than emergency authorization, is beyond me.
Even if one wants to be the most risk-adverse with children and vaccines, how one can be opposed to simple, riskless public health measures such as masking, is something so absurd that it would be unbelievable if read in a fiction novel. Yet that is exactly what multiple governors and school districts are doing.
To quote CMG Pediatrics: “"Grouping unmasked children together in an indoor space for a prolonged period of time dramatically increases the likelihood of viral transmission. Schools that do not require masks are at risk for large viral outbreaks.” And that is exactly what is happening. In Mississippi alone, 4,500 children have tested positive so far. It’s not even September, let alone cold & flu season yet!
Sitting aside children and schools, for adults, the situation is acute. Cases have increased dramatically, hospitalizations are near all-time highs, and these severe cases are translating to deaths. The seven-day average of daily deaths is 1,382. Over 23,000 deaths have occurred in August.

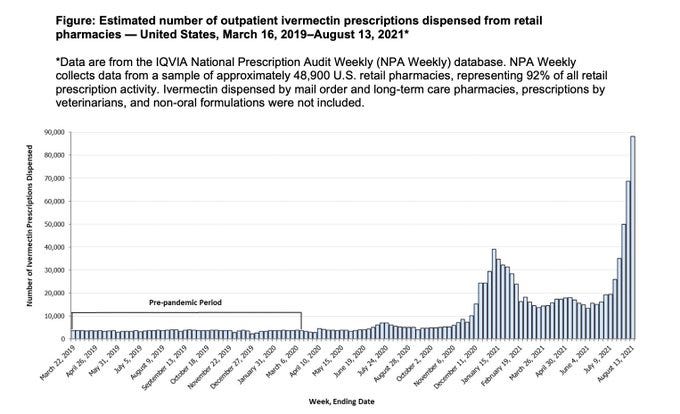
Meanwhile, despite billions of people dosed worldwide with a safe and effective vaccine, certain segments of the American population have decided that Ivermectin, an anti-parasitic used to deworm livestock (it also has some human uses), is the safest option. Outpatient prescriptions for the drug have increased >10x (below) and the CDC has had to issue an urgent health advisory. Over 70% of calls to Mississippi’s Poison Control Center have been Ivermectin related. Multiple states are reporting similar surges.
With increased cases and hospitalizations from COVID-19 and a wave of ivermectin toxicity, hospital systems are overwhelmed in multiple locations. The story broke yesterday that U.S. Army veteran Daniel Wilkinson, of Texas, died of a treatable illness because the COVID crisis left him without an available ICU bed.
The current situation has no easy solution. It requires a combination of vaccination, masking, physical distancing, ventilation, public outreach and education, and coordination among multiple state and federal agencies with local public health and medical organizations. Please continue to wear masks indoors, stay home if you’re feeling ill, focus on ventilation, and encourage family and friends to schedule their vaccination.