

SARS-CoV-2 Update for April 7th
Discussion on various topics, vaccinations continue to scale, comments on herd immunity, reviewing March predictions, plus an Editor's Note.

The Counterpoint is a newsletter that uses both analytic and holistic thinking to examine the wider world. My goal is that you find it ‘worth reading’ rather than it necessarily ‘being right.’ Expect regular updates on the SARS-CoV-2 pandemic as well as essays on a variety of topics. I appreciate any and all sharing or subscriptions.
Editor’s Note: First, apologies for the late newsletter. Life is a bit hectic as my wife and I will be moving from California to Maryland next month. Newsletters may be sporadic throughout April and May, but they will continue! Which leads to the second point. As the pandemic nears an end in swiftly-vaccinating countries, SARS-CoV-2 updates will become much less frequent. COVID-19 will very much remain an issue internationally and I will continue to monitor, but within the United States, there should be very few cases by July, due to a combination of continued vaccinations and strong summer seasonality effects. It’s quite possible that another wave may occur in winter 2021, but assuming continued vaccination campaigns and no clinically-meaningful mutations by the current variants, we’re very near the end of this pandemic. Meaning that this newsletter will transition mainly to the “essays on a variety of topics” mentioned in the intro. For an example, see the first essay : “A Better Way To Lockdown.” If you were here strictly for pandemic updates, feel free to unsubscribe. I’m quite aware how overwhelmed email inboxes can become, so truly, no hard feelings. But I do pledge to make the essays as thoughtful, useful, and interesting as possible.
The fourth ‘wave’ continues but, nationally, it’s more of a plateau. There have been 30,847,926 total confirmed cases of COVID-19 in the United States and the seven-day average of daily cases is 64,731, essentially flat over the last ten days.

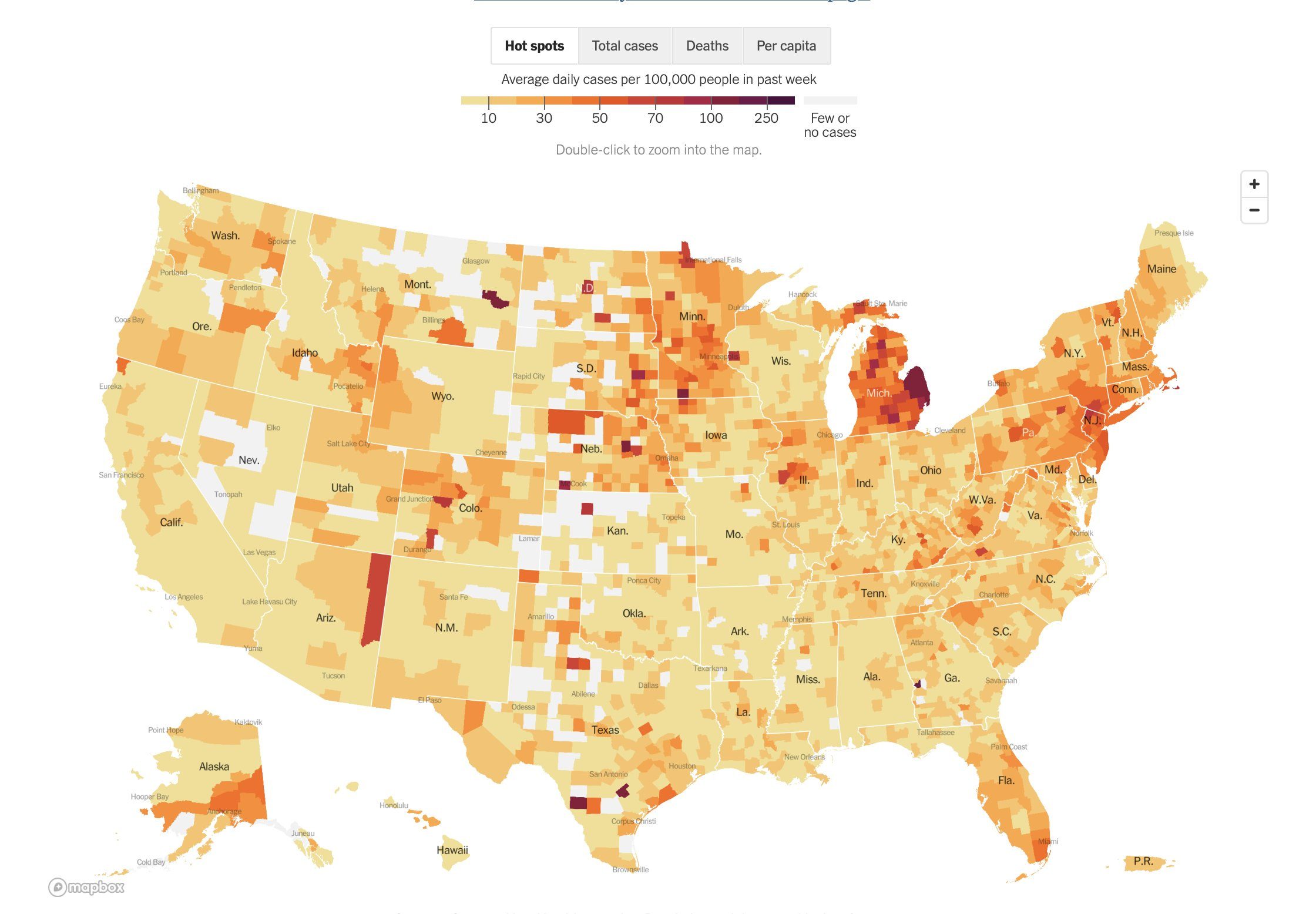
This plateau is a result of a continued surge across colder Northern states offset by continued declines across much of the rest of the country. The wave discussed in the last update continues to build; Michigan is almost back to it’s winter peak! Below is a map of average daily cases per capita. What do the Northeast, upper Midwest, and Alaska have in common? The seasons change much later there!
Fortunately, the correlation between cases and deaths has uncoupled, exactly what you’d expect when you prioritize vaccinations for the most vulnerable. The seven-day average of daily deaths continues to fall and is now at 789, the lowest it’s been since October 24th. There have been 556,529 total confirmed deaths from COVID-19 in the United States.

Brief comments on excess deaths. The Financial Times is out with their latest global excess death numbers. Through the end of February, there were ~50,000 more excess deaths than COVID-19 confirmed deaths in the United States. We’ve long said that because of inadequate testing (and generally poor access to health care) the confirmed death total from COVID-19 in the US should be considered a minimum. But that doesn’t mean that all excess deaths are COVID deaths. For example, both the number of murders and the number of auto accident fatalities increased in 2020. On the other hand (and counter-intuitively) suicides declined by ~6%, according to CDC data published in JAMA this week. This is all to say that ‘death accounting’ is a complex and nuanced field and that the true COVID death toll for the United States is likely between confirmed COVID-19 deaths and total excess deaths.
Vaccinations within the United States continue to scale to new highs. Three million vaccines are being administered per day (with a slight dip because of the Easter holidays). In total, 168.6 million doses have been administered and 76.9% of total supply has been used.

Vaccine reserves continue to increase to new highs. Over 50 million vaccines are ‘sitting in freezers’ waiting to be administered. This massive amount of reserves is why President Biden has accelerated the date for total adult eligibility to April 19th and most states have already opened for all adults. Even at near-record daily vaccination rates, the US has enough reserves for 16.9 days of continued vaccinations, should no additional doses be distributed.

We aren’t close to herd immunity (despite what prominent WSJ opinion pieces claim). The total immunity within a population is a combination of natural infections and total vaccinations. While we have precise vaccination numbers, because of both inadequate testing and asymptomatic infection, the true number of infections has always been higher than the confirmed totals.
By doing broad-based antibody testing within a region, we can estimate the true number of cases within that region. Using local death numbers, we get a local infection fatality rate (IFR). By combining and analyzing IFR studies from various regions, we can estimate the average IFR at the total population level. As we’ve covered previously, that number is ~0.6% (or more precisely: 0.68%. See ‘A systematic review and meta-analysis of published research data on COVID-19 infection fatality rates’).
Since seroprevalence studies have not been performed everywhere but we have relatively accurate death numbers everywhere, it’s more accurate to use confirmed deaths numbers to estimate immunity from infection. With 556,529 confirmed deaths in the United States and using an IFR of 0.6%, we can estimate at total of 92.7 million cases of COVID-19 in the US (556,529/0.006 = 92.7 million).
On the vaccination front, we have those exact numbers. As stated, 168.5 million shots have been dosed. Since the vast majority of vaccines given are the two shot mRNA vaccines, a rough estimation of total people with immunity from vaccine is total doses divided by two, or 84.3 million.
Assuming that no one vaccinated was previously infected (which isn’t true, but let’s assume this ‘best case’ scenario), then the total number of Americans with immunity is 92.7 million + 84.3 million, or ~177 million (see below), well below an reasonable herd immunity threshold.

‘Long COVID’ remains a serious problem but the vaccines(!) appear to be a promising treatment. A large scale study was published in Lancet this week. Of 81 million COVID-19 survivors, 33.6% (!!) were diagnosed with a neurologic or psychiatric illness within six month of COVID-19 recovery. Of course, some of this just the ‘natural rate’ of such diseases in the population, especially during a rather difficult year, but this is such a large incidence of disease that it should be extremely clear that ‘Long COVID’ is a very real phenomenon.
Fortunately, many ‘long haulers’ are reporting a large reduction in symptoms after vaccination. While the exact mechanisms of both ‘Long COVID’ itself and this alleviation of symptoms remain unknown and unresolved, the mental model that seems to be emerging is the herpes simplex virus (herpes simplex 1 causes cold sores and herpes simplex 2 causes genital sores).
Both herpes viruses have methods of evading the immune system. So while our immune systems can completely control the disease, it can never fully eradicate the virus. For example, with herpes simplex 1, the virus hides in the epithelial cells of the mouth, and every once in awhile when the immune system is weakened, the virus will re-emerge and cause a cold sore.
A similar phenomenon might be what is occurring with SARS-CoV-2. For most infected patients, their immune system fully eradicated both the disease and the virus. But in a subset of patients, for some unknown reason, the immune system isn’t strong enough to remove every last bit of virus and that surviving virus ‘goes into hiding’ in the tissues that it can infect (many tissues express the ACE2 receptor including the lungs, intestines, heart, and brain). The next time the immune system is weakened, one of these pockets of virus emerges and causes a ‘cold sore.’ The problem is that herpes simplex infects external tissues so we can see those sores, but since SARS-CoV-2 infects internal tissues so we can’t directly the damage from this viral reemergence. As the immune system concentrates on whatever tissue breaks out first, this provides an opening for another pocket of virus in another tissue to emerge. Thus the immune system is in a constant state of ‘CoV-2 whack-a-mole,’ which is why these patients continue to suffer chronic symptoms for months on end.
Where the vaccines come in as a potential ‘cure’ is that the entire point of a vaccine is to stimulate the immune system to better detect, respond to, and eliminate a pathogen. When Long COVID patients are vaccinated, what seems to be happening is that their immune system gains enough power that it can fully eradicate the pockets of SARS-CoV-2 that have hidden themselves around the body, the ‘whack-a-mole’ stops, and the ‘cold sores’ all over the internal tissues resolve, finally repairing themselves.
To reiterate, the exact mechanisms surrounding Long COVID are unknown. But if you know someone suffering from it, please recommend vaccination to them.
Reviewing March Predictions
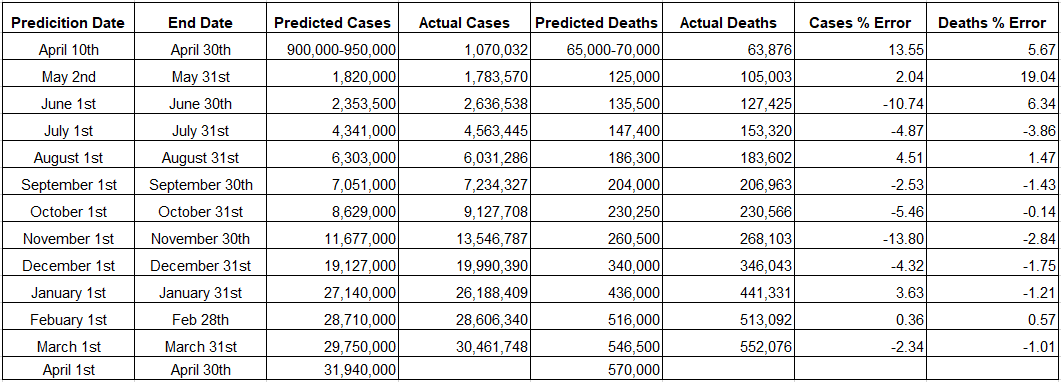
On March 1st, I predicted at the end of March, there would be 29,750,00 confirmed cases and 546,500 confirmed deaths in total. On the morning of April 1st, there were 30,461,748 confirmed cases and 552,076 confirmed deaths.
Both of my March predictions were below the true values as I completely missed the ‘fourth wave.’ I believed that the large numbers of vaccinations would keep cases at bay. Specifically, my model “starts the month at 400,000 weekly cases and ends the month at 200,000 weekly cases.” Unfortunately, we haven’t vaccinated quite as much as Israel or the United Kingdom (which have seen continued declines) leaving room for a minor surge in cases in our norther states. We ended March at ~470,000 weekly cases, a slight increase over the month. Since cases and deaths have been highly correlated, it makes sense that underpredicting cases would also mean an underprediction in cases.
Moving forward, continued vaccination campaigns combined with daily increases in seasonality effects means I’ll continue to predict a decline in cases. On March 30th, I voted for ‘40k cases per day’ in Nate Silver’s poll on the average of daily cases on May 1st. On March 1st, the seven-day average of daily cases was ~67,000 and getting to 40,000 daily cases by May 1st, means ~1.5 million cases in April, or 31,940,000 total confirmed cases at the end of April.
As stated earlier in the newsletter, cases and deaths have finally decoupled. Thus our previous heuristic (a 1.7% CFR on a 21-day lag) will no longer work. Using a simple trend model that ends April at 500 deaths per day means ~18,000 deaths in April, or 570,000 total confirmed deaths at the end April.
If you enjoyed The Counterpoint, please share, subscribe, or comment below.