SARS-CoV-2 Update for Jan 4th 2022
The final stage of the pandemic, the beginning of the endemic.

The Counterpoint is a free newsletter that uses both analytic and holistic thinking to examine the wider world. My goal is that you find it ‘worth reading’ rather than it necessarily ‘being right.’ Expect regular updates on the SARS-CoV-2 pandemic as well as essays on a variety of topics. I appreciate any and all sharing or subscriptions.
Globally and within the United States, SARS-CoV-2 is spreading faster than at any previous point in the pandemic. The evidence has solidified that the Omicron variant is both significantly more transmissible and has meaningful capacity to evade prior immunity, either from natural infection or vaccination. It will not be today nor tomorrow, but each and every one of us will be infected by SARS-CoV-2. We are in the final stage of the pandemic; the time of the endemic is beginning.
Endemic does not mean SARS-CoV-2 goes away, but rather the opposite: it will be the fifth coronavirus (and ~200th respiratory virus) that circulates indefinitely through the human population.
Endemic does not mean SARS-CoV-2 isn’t a threat. Even after we’ve all been infected, vaccinated, or both, COVID-19 will continue to hospitalize and kill people. Below is a graph of weekly confirmed influenza deaths in the United States from 2010 through early 2019.1 In the United States, influenza averages ~35,000 deaths annually. Annual COVID-19 deaths will depend on a number of factors, but they’re likely to be in the 40,000 to 100,000 range for the immediate future. These deaths will be highly concentrated in the elderly, immuno-compromised, those with co-morbidities, and unvaccinated.

What endemic SARS-CoV-2 does mean is that we will have to ‘learn to live with the virus.’ But to be explicit, this does not mean we do nothing and just let respiratory viruses spread through communities every winter. Endemic SARS-CoV-2 means a change in strategy and a shift in responsibility.
When cholera was first discovered and it’s transmission (contaminated water) determined, we didn’t just go: ‘oh well, diseases happen, nothing we can do.’ Nor did we ask individuals to carry water filtration units and manage their own sewage. What we did do was massive public investment by government and public health institutions to upgrade water and sewer systems, set water quality standards, and start educational campaigns about cholera and it’s source.
A similar shift to institutional responsibility is necessary for SARS-CoV-2. We cannot ask individuals to mask forever. We cannot ask individuals to physical distance forever. We cannot have children in-and-out of school forever. We need our institutions to step up and start evidence-based public health measures that can remain in place for the long term. These should include:
Investment by local, state, and federal governments to increase ventilation and sanitization of indoor air in all public buildings.
Direct investment or tax credit/rebate for individual households to increase ventilation and sanitization of indoor air in private residences.
Updating and setting modern air quality standards, both indoor and outdoor.
Investment and empowerment of internal government agencies involved in pandemic detection and prevention.
Investment in local and state public health departments so that testing capacity, both the collection and processing of samples, can be maintained indefinitely.2
Education and outreach campaigns, both targeted and broad-based, by local and state public health departments about the importance of vaccines and staying home when ill.
Mandatory sick leave policy for all workers, regardless of hourly or salary.
None of these place responsibility on the individual or families, all are policies that can remain in place permanently, and all are policies that resemble those that we used in previous centuries to control food- and water-borne diseases. These measures will minimize not just SARS-CoV-2 but also other respiratory illnesses, such as influenza and asthma, which cost the US ~$11 billion and ~$80 billion annually, respectively.
Of course, these will not occur overnight and will require both long-term political pressure and public funding.
The Current State of Affairs
Confirmed COVID-19 case numbers, both globally and within the United States, are at never-before-seen numbers. The Omicron variant is highly transmissible, has a significant capacity for evading prior immunity, winter temperature and humidity generally promotes respiratory virus transmission, and compliance with non-pharmaceutical interventions is lackluster. All this compounds into exponential growth. Globally, the seven-day average of cases is at 1.627 million. Within the US, it is at 477,306.


Both of these should be considered severe undercounts. Within the United States, it’s likely that there are >1 million cases per day. Our testing volume remains wholly inadequate. The current positivity rate is >20% nationally (below, source: Johns Hopkins). Undoubtedly, the current wave is much larger than confirmed numbers. It would not be surprising if 30-50% of Americans are infected during December, January, and February.

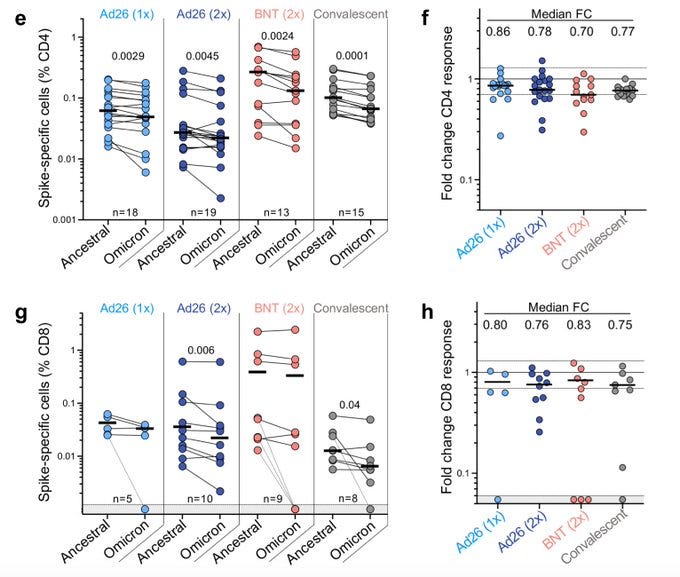
The vast majority of these infections will be mild. Even if prior immunity is evaded, it continues to protect from severe disease. While Omicron’s mutations allow it to avoid neutralization by antibodies, our immune system has multiple layers of defense. Multiple studies (one, two, three) suggest that our T cell response remains robust3. Best image shown below, comparing CD4+ and CD8+ T cell populations in J&J (Ad26), Pfizer (BNT), and previously infected (convalescent) patients.
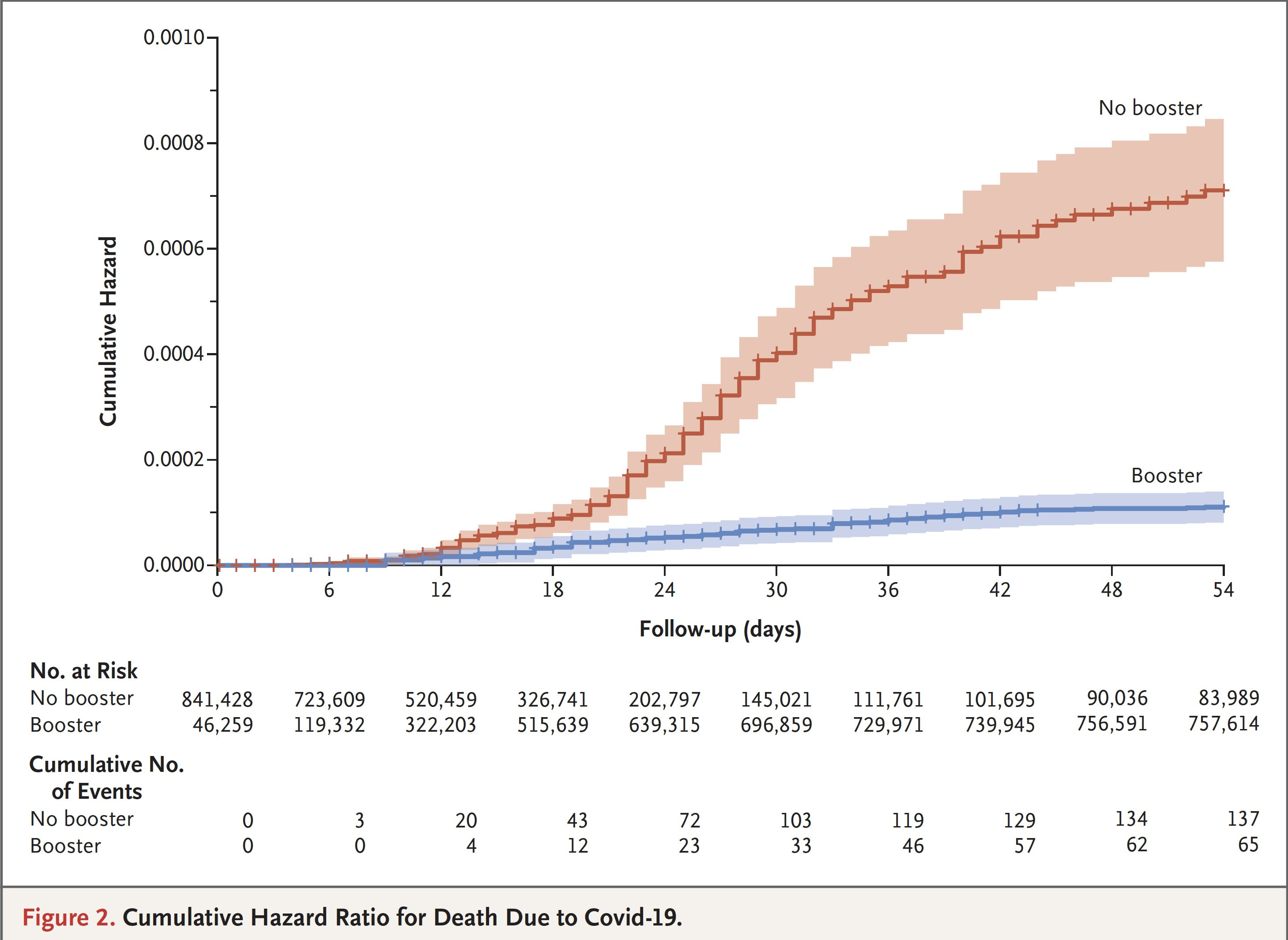
Clinical and laboratory assays measuring neutralizing antibodies, T cell responses, etc., can be abstract. Not everyone cares for scientific figures or underlying mechanisms. To get down to the brass tax, the best way to protect yourself is to schedule your booster vaccination. Below is an image of cumulative deaths in a cohort of 840,000 individuals as they were tracked by the Israeli Ministry of Health (published in NEJM). Participants who received a booster (blue line) had a ~90% lower mortality due to Covid-19 than fully-vaccinated participants who did not receive a booster (red line). This is a ~90% reduction on top off the ~90% reduction the initial two doses of vaccine provides. This is the type of graph that “needs no statistics.”4
The issue is that a large portion of the United States has no prior immunity, either from vaccination or infection. The massive surge in cases is causing an increase in both hospitalizations and ICU admissions (below, top). Now, there is some truth to the ‘hospitalized with COVID’ vs ‘hospitalized for COVID’ distinction. With such a large wave of cases, many people that go to the hospital for various other reasons will also incidentally be infected with SARS-CoV-2. Some states are beginning to make this distinction in their reporting.

Regardless of this distinction, hospitals are still strained and the vast majority of these hospitalizations are the unvaccinated. According to Governor Larry Hogan (Republican, Maryland): “the 8% [of adults in MD] who remain unvaccinated account for 75 percent of hospitalizations.” Recently, he declared a 30-day state of emergency and mobilized the Maryland National Guard to help bolster testing and hospital capacity.
Tens of Thousands of Americans Are Dying
People interpret both cases and hospitalizations in various ways (below image credit to Dr. Eric Topol). And they should; it is a complex situation with lots of caveats. What isn’t complex is that 45,966 Americans died from COVID-19 in December. That is just below 1,500 per day. Nearly all of them were unvaccinated.

We are profoundly failing as a society. I have neither answers nor solutions on how to reach the remaining unvaccinated. But the data is clear that it is the unvaccinated who are dying. Vaccine hesitancy killed hundreds of thousands of Americans died in 2021. Even conservative estimates predict ~150,000 additional deaths from the Omicron wave. Know that it is never too late to schedule your COVID-19 vaccination.
Does Omicron Cause Milder Disease
The evidence does suggest that Omicron does cause milder disease. This took some time to sort out because there were many confounds, mainly, a substantial level of prior immunity. A way to think about this is when the Europeans came to the New World, smallpox didn’t suddenly become more deadly. It just entered a population with no immunity. The reverse was true for Omicron; it enters first entered into a population with lots of prior immunity,5 so it should have an observed fatality rate that is lower.
But after accounting for the various confounds, the data does suggest Omicron causes milder disease, especially compared to Delta. The underlying biological reason for this is that Omicron seems to have difficulty infecting lung cells, preferring rather the epithelial cells that line the upper airways. A summary of these studies can be found here. Moreover, it may have even switched its mechanism for infecting cells.
This doesn’t mean Omicron isn’t a threat. Even if it’s half of severe, if it’s transmissible enough that cases double, that means the same number of severe cases and death. To put some concrete math on it, ~1/3 of Americans remain unvaccinated. The IFR of ‘wild-type’ SARS-CoV-2 is ~0.6%. Using half severity and 50% of Americans getting infected in the next few months, that would mean ~164,000 additional deaths from just the unvaccinated portion of the population.6 And while the vaccines are highly effective, they are not 100.0% effective at preventing hospitalization and death, especially in the elderly, immuno-compromised, and those with co-morbidities.
Omicron is spreading rapidly. Though it appears to cause milder disease, there are so many cases that hospitals are filling. With the United States’ subpar vaccination rate, we should expect elevated death tolls through winter. The best way to protect yourself and loved ones is by scheduling your primary vaccination or booster.
Notice that the seasonal pattern for influenza is quite clear, sometimes shifting by several weeks sooner or later, but always starting between late fall and mid winter in the Northern Hemisphere. In the Southern Hemisphere, it starts in the Northern Hemisphere’s late spring to mid summer. In the Tropics, there is very little seasonal pattern. Not all diseases display seasonality and not all that do display seasonality concentrate on the winter. While seasonality is a clear phenomenon for many diseases, the underlying cause for the pattern is only poorly to moderately understood. If interested, you can read more here and here.
Pfizer’s antiviral pill, Paxlovid, requires beginning treatment within five days of the first symptom, and the earlier the better. For Paxlovid to be effective, we will need COVID-19 testing, with results delivered quickly, for the indefinite future.
Further evidence for this is that the T cell response remained robust against the Beta variant, the other variant with significant immune evasion capacity.
While South Africa didn’t have a super high vaccination rate, it seems most people underestimate how widespread prior waves of SARS-CoV-2 hit the nation. South Africa has 414 excess deaths per capita, compared to 333 excess deaths per capita for the United States, the hardest hit first-world nation.
330,000,000 American population * 0.33 unvaccinated * 0.5 infection rate * 0.003 IFR = 163,350 deaths