

SARS-CoV-2 Update for September 18th
The Delta variant is stalling but with the United States' inadequate vaccination rate, winter looms.

The Counterpoint is a free newsletter that uses both analytic and holistic thinking to examine the wider world. My goal is that you find it ‘worth reading’ rather than it necessarily ‘being right.’ Expect regular updates on the SARS-CoV-2 pandemic as well as essays on a variety of topics. I appreciate any and all sharing or subscriptions.
Case counts in the original hotspots of the Delta variant, such as Florida and Louisiana, are descending, yet new ones, all with below-average vaccination rates, are facing a new wave of cases. Tennessee, Kentucky, Idaho, and North Dakota all have rapidly rising case counts. The most vaccinated of these four is Tennessee, with only 50.5% of it’s population fully vaccinated.

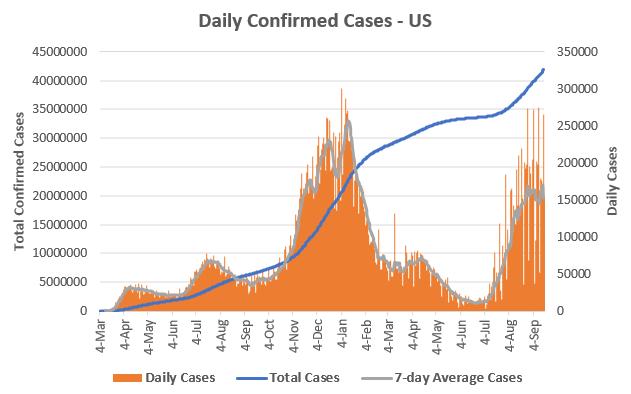
Nationally, this mix causes case counts to form a rough plateau. With some states falling, some states rising, the United States has been between 150,000 and 170,000 daily confirmed cases since August 24th. There have been 41,930,539 total confirmed cases in the US.
Fortunately, despite the plateau in cases, it appears that hospitalizations have peaked and continue to decline slightly. To be clear, with 89,181 Americans currently hospitalized and 24,893 in the ICU, we are still deep into the second largest wave of COVID-19. Individual states continue to suffer, for example, both West Virginia and Idaho hospitalizations are at all-time highs. The situation in Idaho is particularly acute; the state is allowing hospitals to ration care and hospitals in Washington state are feeling the pressure from transferred patients and Idahoans that simply drive themselves over the border.

As with every previous wave, deaths follow hospitalizations, on a slight lag. The United States is back above 2,000 deaths per day. In total, 672,024 Americans have died from COVID-19. 32,336 of these have been in September 2021.

The worst part of the present situation is that is was entirely preventable. On June 1st, the United States was one of the most vaccinated nations in the world (below). Today, despite multiple readily-available and monetarily-free vaccines, with overwhelming data supporting their safety and efficacy, we are one of the least-vaccinated first-world nations. Assuming current vaccination rates continue in Australia, New Zealand, Japan, and South Korea, we will soon be the single least-vaccinated first-world nation.

This was not because of vaccine supply issues. Vaccines reserves are currently at all time highs of 78.4 million (over 100 days supply at the current vaccination rate). Since April 7th, they’ve never dipped below 50 million, despite the Biden administration shipping over 100 million doses abroad.

This lack-of-vaccination is solely because, collectively, we’ve refused to ‘get shots in arms.’ Our vaccination campaign peaked in mid-April and has slowly bled down to the current trickle of ~770,000 shots per day. Only 54.2% of Americans are fully vaccinated and 63.5% have at least one shot. Worse, these numbers overstate the case, considering that many people have voluntarily went and gotten ‘off-the-books’ booster shots.

This is all due to an absurd mix of misinformation, propaganda, mistrust in public health, and politicization of the science. All available evidence suggests the vaccines continue to provide robust protect from hospitalization and death, with moderate reductions in symptomatic disease.
No matter how you slice the data, whether intra-state (credit NYT)…

…between states (credit NYT)…
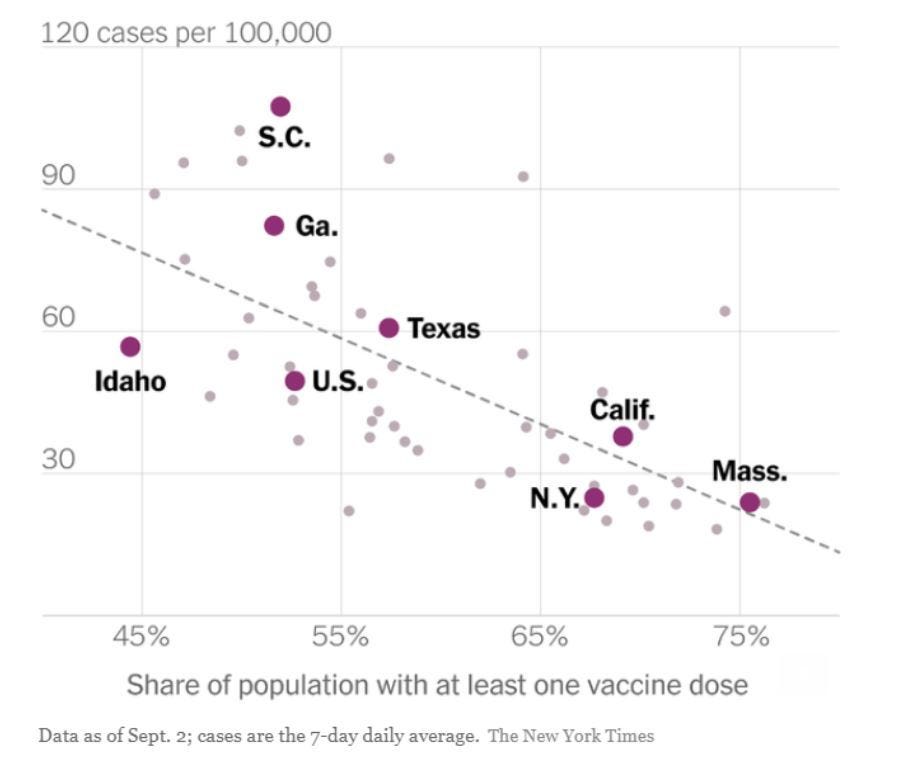
…in other countries (credit FT)…

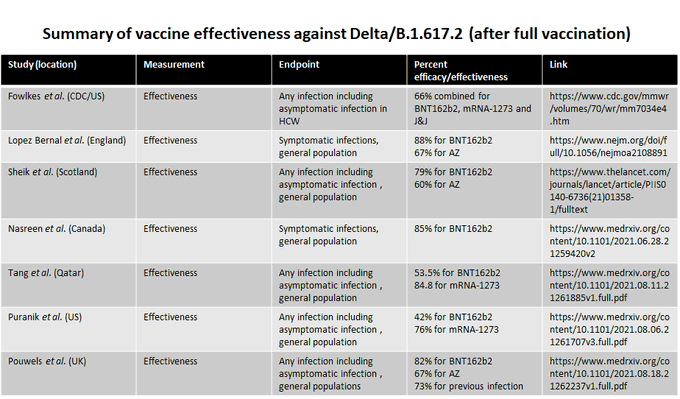
…or simply look at the numerous clinical trials of vaccines vs. the Delta variant (below, credit to Dr. Florian Krammer). It bears repeating over and over and over. The vaccines work, the vaccines work, the vaccines work.
Obviously, the future is unknown. But there is moderate-to-strong evidence that the situation is will worsen as we move into winter.
The reproductive number, also known as Rt, is an epidemiologic metric describing the contagiousness or transmissibility of infectious agents. If Rt = 1, then, on average, an infectious person will infect one other person. In this situation, cases would remain flat, since one infection leads to one more. If Rt > 1, case counts increase; if Rt < 1, case counts decrease.
Many factors influence the transmissibility of a virus. Obviously, the more people that carry immunity, whether through prior infection or vaccination, this will decrease Rt, since the virus will have less opportunity to encounter a susceptible person. Likewise, a decrease in ‘social connectivity,’ whether through voluntary physical distancing/isolation or mandatory quarantines/lockdowns1, will decrease Rt.
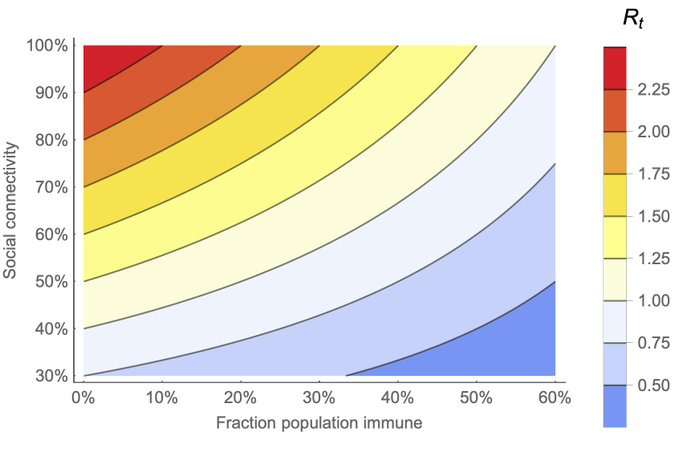
Considering both these variables, population immunity and social connectivity, one can construct a graph of Rt2 (below, credit to Dr. Trevor Bedford, a virologist at the Hutch Institute.)
But transmissibility is influenced by more than just population immunity and social connectivity. For example, different variants can have different innate contagiousness. For example, consider two populations that have the exact same level of immunity and connectivity, with the original CoV-2 variant infecting one and the Delta variant infecting the other. The population infected by the Delta variant would end up with more cases.
Seasonality is also an important influence on Rt. Temperature and humidity influence how viruses spread. This ultimately results in our annual ‘cold & flu’ season during the winter (in the Northern Hemisphere). Phrased differently, at a constant immunity and constant connectivity, Rt increases during the winter.
We’ve only lived through one winter with SARS-CoV-2 but it’s extremely likely that is displays seasonality. All four endemic human coronaviruses exhibit a seasonal pattern (below) with cases rising in October, peaking in December, and trailing off through the spring. This would explain why our largest wave of COVID-19 started in September 2020, peaked in January 2021, and trailed off through spring 2021.

Where this comes to a head is that there will soon be multiple forces pushing Rt higher. With re-openings, connectivity is returning to ~2019 levels, putting upward pressure on Rt. The coming winter weather will also put upward pressure on Rt.
Meanwhile, vaccination rates have stalled, meaning that any downward pressure on Rt from increased immunity is coming from naturally-occurring cases, which all else being equal, we should want to avoid.
Will 54.2% of Americans being fully vaccinated be enough to keep Rt < 1 during the winter months? That is unknown3. But the more-transmissible Delta variant combined with continued re-openings, winter weather, and stalling vaccination rate does not bode well for the coming months in the United States.
Questions about the effectiveness of lockdowns relates to their practical implementation, not whether they ‘work.’ If we’d all stayed in our homes, and only our homes, for the entirety of March 2020, there wouldn’t have been a pandemic. But everyone staying in their homes, and only their homes, is obviously unrealistic. The question is whether enough people reduce their social connections enough of the time to reduce Rt. Here is a very detailed and well-citied post, by Substack writer AstralCodexTen, that concludes, “Various policies lumped together as “lockdowns” probably significantly decreased Rt.” Whether this reduction of R0 is worth the economic and psychological costs is a separate and important question. Of course, costs and benefits change over time. In 2020, these costs were probably generally worth it. In 2021, these costs probably aren’t.
This graph was published when the D614G variant was predominate. Thus at 0% immunity and 100% connectivity, Rt is ~2.25. With the evolution of the Delta variant, baseline Rt is on the order of 5-9, probably on the lower range.
To get some idea, I’d watch European case counts closely, especially Denmark, which recently removed *all* COVID restrictions. Denmark has a much higher vaccination rate than the US. If they start to have a winter wave, we should too. If they do not, our fate remains uncertain, since we have a much lower vaccination rate.