

mRNA Vaccines and Myocarditis
A brief Omicron update followed by an examination of the risks from mRNA vaccines.

The Counterpoint is a free newsletter that uses both analytic and holistic thinking to examine the wider world. My goal is that you find it ‘worth reading’ rather than it necessarily ‘being right.’ Expect regular updates on the SARS-CoV-2 pandemic as well as essays on a variety of topics. I appreciate any and all sharing or subscriptions. You can follow me on Twitter @PatrickHeizer
Omicron: a Tough Path to Endemicity
The Omicron wave continues to spread at unprecedented rates. A highly-transmissible variant + a significant capacity to evade both naturally-acquired and vaccine-acquired immunity + winter’s temperature, humidity, decreased ventilation, and social patterns + reduced compliance with non-pharmaceutical public health interventions = a “textbook” epidemiological case curve.

Fortunately, the Omicron wave appears to have peaked within the United States. The seven-day average for confirmed cases peaked on January 16th at ~804,000. It is currently ~726,000. At these confirmed case levels and test positivity rates, ~1% of the total United States is being infected per day. Dr. Trevor Bedford estimates 36-46% of Americans will have been infected by Omicron by mid-February (below). In the January 4th update, I estimated 30-50% of the US would be infected by the end of February. This may end up a slight underestimate.

The totality of evidence is clear that vaccinations continue to provide protection against Omicron and that a third dose is essential for maximum protection. The following data are mostly from four major reports. Though from separate entities, they are remarkably consistent with each other. These four are from the UK Health Security Agency, Kaiser Permanente of Southern California, the CDC’s MMWR, and the Qatar Ministry of Health.
The Omicron variant is indeed milder but not “mild.” The below data is from Kaiser Permanente (not the best labels but “SGTF”/green is Omicron and “No SGTF”/purple is Delta). Omicron causes less hospitalization, ICU admission, and mortality than Delta. But remember that Delta was a significant increase in severity and that there is now much more immunity (both naturally- and vaccine-acquired) present in the population. Once you control for these confounds, Omicron is ~25% less virulent than Delta, meaning it is roughly as virulent, perhaps slightly less, as the original strain.1

The vaccines are still somewhat protective against infection. Because of all the breakthrough infections, it may seem like the vaccines do not protect from infection. While there has been a clear reduction from the 90-95% protection from infection seen in the original 2020 clinical trials, boosters shots appear to provide a 50-66% reduction in symptomatic infection. Summary image credit to Dr. Eric Topol.

Most importantly, the vaccines remain incredibly protective against hospitalization and serious disease. Having the third booster dose decreases your relative risk of hospitalization by an order of magnitude. Summary image credit to Dr. Eric Topol.




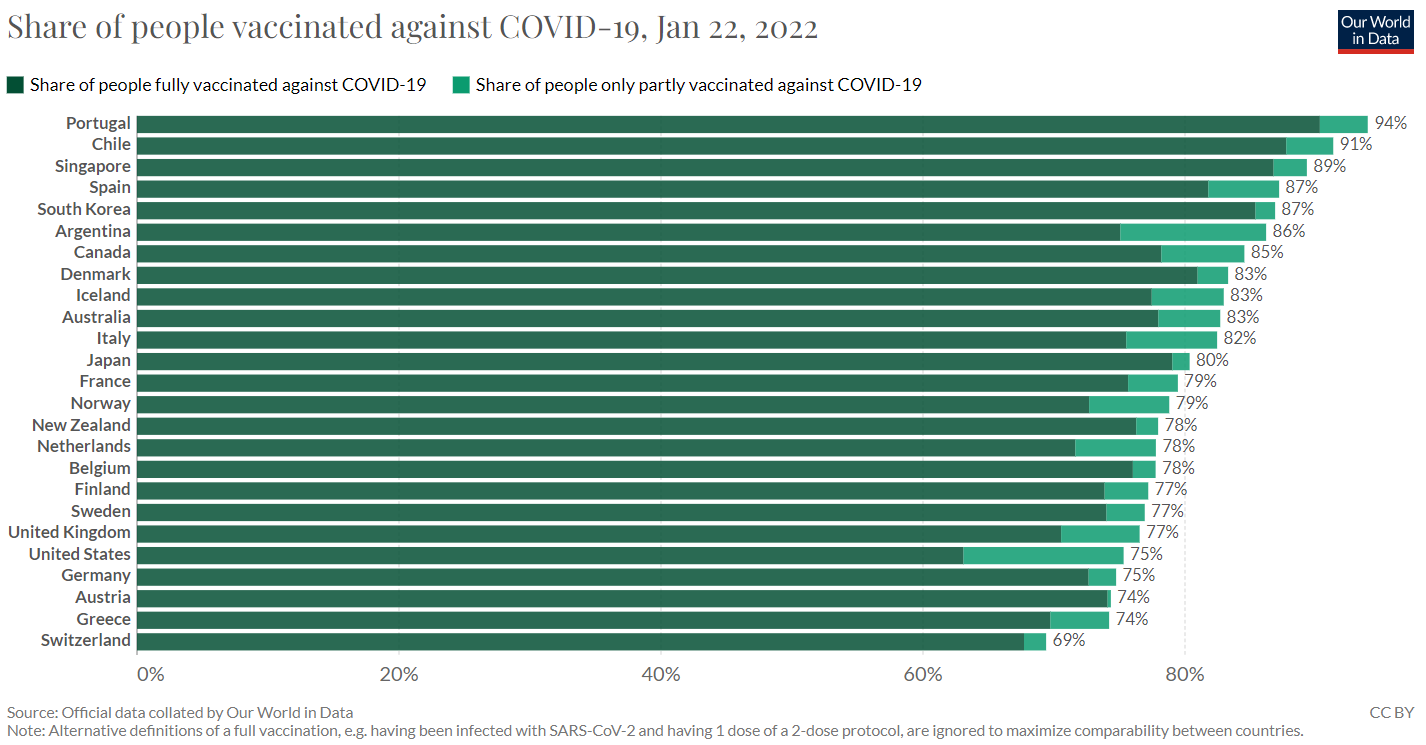
Despite their clear benefit, the issue continues to be that the United States remains significantly less vaccinated compared to other first-world nations. Below are 25 nations from various geographies. The United States ranks 25th out of 25 in terms of percentage of its population that is fully vaccinated.
Consequently, the United States continues to have many COVID-19 deaths. The seven-day average of daily confirmed deaths is 2,178. A total of 39,763 Americans have died in January 2022, or 1,807 per day. This month is on pace to be a top-five deadliest month of the entire pandemic.

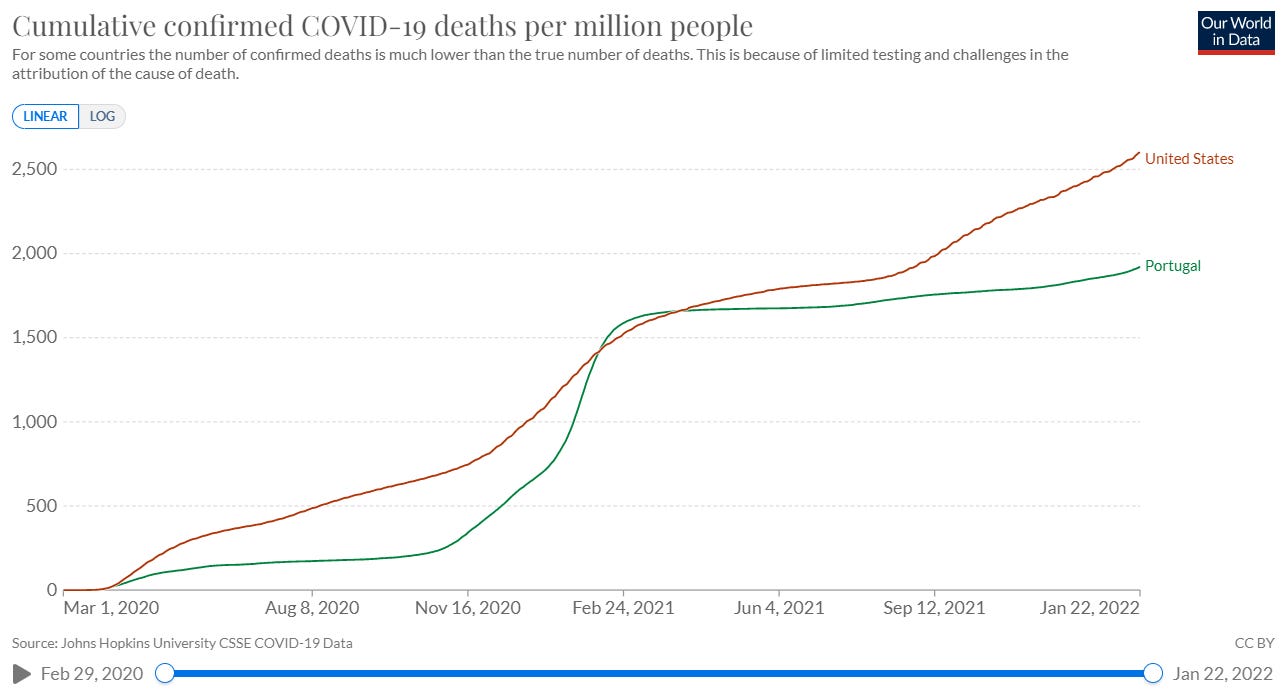
Case Study: Portugal vs. the US
Of the 25 nations in the chart above, Portugal is the most vaccinated. Comparison to the United States below.

On April 1st, 2021, Portugal and the United States both had 1,660 cumulative confirmed deaths per million. Today, the United States is at 2,598 cumulative deaths per million, compared to 1,917 for Portugal, or an additional ~700 deaths per million for the United States. Assuming ~330M US population, that is ~231,000 Americans that would be alive if we’d had Portugal’s death rates.
mRNA Vaccines & Myocarditis
The COVID-19 pandemic has been a real-life course in risk. Individual vs population risk, linear vs exponential growth, complement vs substitution effects, cost vs benefit analysis, counterfactual comparisons, etc.
All medical procedures carry some risk. Whenever one is performed, it is because a patient and their physician have decided that the potential benefit outweighs the potential risk. These benefits and risks can vary between people.
Because SARS-CoV-2 is an endemic virus, we all will encounter it at some point. Thus the proper comparison for any risk from vaccination is one’s risk from COVID-19. With the mRNA vaccines, the most discussed risk is myocarditis (inflammation of the heart muscle). This has rightfully been investigated as myocarditis can be serious.
The two best studies of the myocarditis risk from vaccination are Patone et al. (published in Nature Medicine December 2021) and Husby et al. (published in BMJ in December 2021).
These studies caused a stir as both found an increased risk of myocarditis following mRNA vaccination than from CoV-2 infection. Woah! But while that previous sentence is technically true, it excludes some very important context and considerations.
First, the risk of myocarditis is isolated to only younger people that have taken two doses of the Moderna (mRNA-1273) vaccine2. The below figure from the Patone paper circulated rapidly on social media. While COVID-19 caused 10 excess events per million of myocarditis in those under 40 years old, the second dose of Moderna caused 15 excess events per million, a ~50% relative increase.
But one’s interpretation shouldn’t be “mRNA vaccinations cause myocarditis,” but rather “we should recommend only the Pfizer mRNA vaccine to adolescents and young adults.” And that is exactly what France, Germany, and other nations have done.

Moreover, the above image is cropped. Very rarely is the full figure from the paper shown (below). Myocarditis is not the only cardiac side effect from either vaccination or CoV-2 infection! If you include pericarditis and cardiac arrhythmia, it’s clear that the total cardiac risk of CoV-2 is exponentially higher than from vaccination.

And that is just cardiac risk! Other major concerns from CoV-2 infection are both short- and long-term lung and brain injury. There is no evidence that mRNA vaccination causes either of these. mRNA vaccines do have other moderate risks, such as allergy, but all occur at very low rates.
Finally, there can be a false equivalence when interpreting these myocarditis cases. These papers merely counted “events.” I.e. both a mild and a severe myocarditis case counts as an event. The vast majority of vaccine-related myocarditis were mild and patients recovered quickly. For COVID-19, not only can it cause severe disease in the short-term, but it’s increasingly clear that “Long COVID” is a real phenomena3 and that vaccines reduce the risk of it (below image from a preprint published last week).

Factoring in the totality of the various risks (myocarditis, allergy, etc for mRNA vaccination and myocarditis, pericarditis, lung damage, nervous system damage, death, etc. for COVID-19), it’s clear that the total risk of COVID-19 far outweighs the total risk from mRNA vaccination.4
To put numbers on these, infection fatality rates are estimated to be ~0.6% for the original strain, ~0.8-0.9% for Delta, and 0.5-0.6% for Omicron. These numbers are for **an immune-naive** population and at the total population level. One’s individual risk is highly dependent on one’s age and co-morbidity status. Having prior immunity, either from previous infection or vaccination, further reduces one’s individual risk by ~90%
Even more precisely, it’s primarily adolescent and young adult biological males.
It’s also clear that “Long COVID” does not occur at rates previously feared. My reading of the literature is that the true percentage of people that have true long-term side effects from COVID-19 is on the order of 1-5%. We should all recognize these patients, investigate the underlying biological mechanisms, and work to develop treatments for this post-viral syndrome.
If you are <30 years old and have the option, I would suggest that you chose the Pfizer vaccine, especially if a biological male. This is not because Moderna is “unsafe” but you have to reduce risk where you can, and it’s clear that Pfizer causes less myocarditis than Moderna, possibly because it is ~1/3rd the dose of mRNA.