

Our Immune Systems Weren't Damaged by SARS-CoV-2

The Counterpoint is a free newsletter that uses both analytic and holistic thinking to examine the wider world. My goal is that you find it ‘worth reading’ rather than it necessarily ‘being right.’ Expect regular updates on the SARS-CoV-2 pandemic as well as essays on a variety of topics. I appreciate any and all sharing or subscriptions.
You may have encountered media that SARS-CoV-2 chronically damages the human immune system.1 For an example of a ‘mainstream’ article, see the Forbes article “SARS-CoV-2 Actively Infects And Kills Lymphoid Cells.”
But despite a slew of scientific articles and media attention claiming widespread immune damage, it’s clear that our immune systems are fine.
If a meaningful number of people were chronically immunocompromised from SARS-CoV-2 infection, there would be substantial changes in the epidemiology of human diseases, both increased frequency/morbidity of regular human disease and/or increased frequency/morbidity of opportunistic infections.
And there are no signs of this occurring.
Patterns of Infectious Disease Have Been Normal
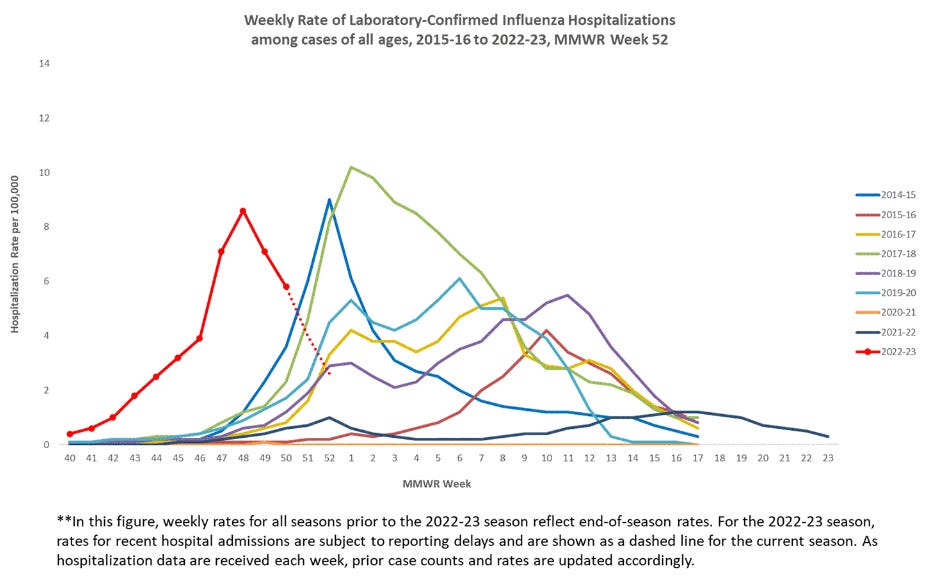
Influenza is a respiratory disease with annual winter waves. On average, ~35,000 Americans die per year from influenza. In 2023, while the wave increased earlier-than-usual, all signs suggest it is normal in magnitude and severity. Weekly total hospitalization rate (top) and weekly pediatric deaths (bottom) are shown below. Influenza vaccines are widely available and typically free-of-charge.

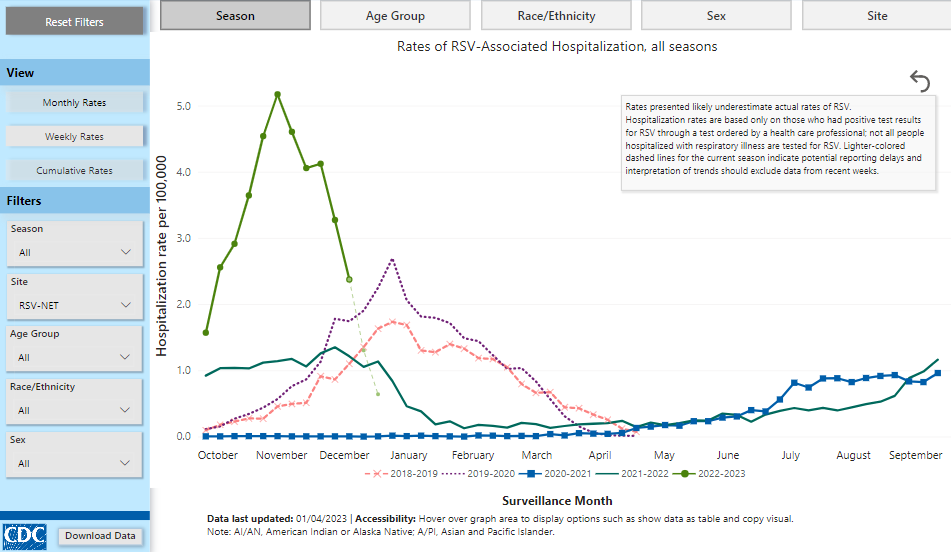
Respiratory Syncytial Virus is another respiratory virus with annual winter waves. Just like influenza, RSV spread earlier-than-usual. While it’s magnitude of hospitalizations was greater, the difference in peak hospitalization rate between the 2019 season and 2022 season was ~2.5 hospitalizations per 100,000. This is after two consecutive very mild years (2020 and 2021). RSV vaccines are in late-stage development and are likely only a couple years away.
SARS-CoV-2 needs no introduction. While hospitalizations have been ticking up, this is almost entirely due to those over the age of 70. Age has always been the number one risk factor for severe COVID-19. Less than 40% of the elderly have received their bivalent booster shot which is ~80% effective at preventing hospitalization. In younger cohorts, immunity from vaccination and/or infection remains robust.

Monkeypox is a virus that doesn’t typically spread in the United States. When the outbreak begin, some asserted that this was likely due to damaged immune systems. The virus spreads also exclusively through sexual contact and health authorities targeted education, outreach, and vaccination. Cases have fallen to near zero

Acute flaccid myelitis (AFM) is an uncommon but serious neurologic condition. While it’s exact etiology is unknown, it’s believed to be viral, as ~90% of cases a preceded by a viral infection of some type. Pre-pandemic, it displayed an every-other-year pattern. Cases have remained low since 2018.

A wave of childhood hepatitis of unknown cause occurred in 2022. While it is still being looked into, the total number of cases under investigation (so not total confirmed) is only 384.

Measles is the most contagious virus known. There is currently a large cluster outbreak in Ohio. 67 of the 73 patients were unvaccinated.
Scarlet fever, caused by Group A Streptococcus bacteria, has seen a significant increase in cases in 2022. What is rarely mentioned is that scarlet fever cases increased ten-fold between 2000 and 2016. See this commentary in Lancet or this article in Vox, both from 2017. Despite this, the 2022 outbreak has been especially large in certain nations like the United Kingdom. The CDC has issued a health alert and it’s surveillance can be found here.
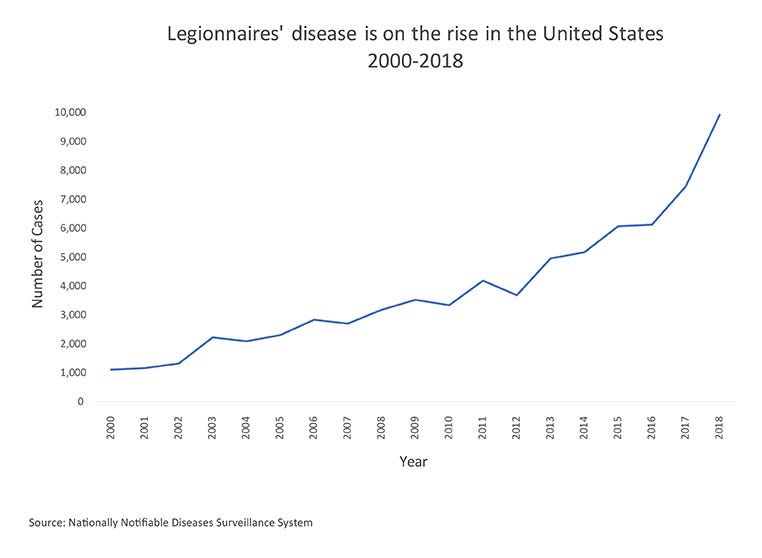
Legionnaires’ disease, caused by Legionella bacteria, is mainly spread through water. Some have attributed Legionella outbreaks in 2022 to damaged immune systems. But just like scarlet fever, they neglect to mention that its incidence began rising many years prior to the pandemic.
The Difference Between Science and Clinic
The point of the above section is that the epidemiology of infectious diseases in 2022 has been, roughly, normal, which is not what we’d expect if millions of people became chronically immunocompromised after SARS-CoV-2 infection.
So how did this theory start and spread?
In “Pandemic Lesson #2: The Complexity Ocean,” I listed “the production, dissemination, and interpretation of scientific knowledge” as one of the complexities of the modern age. The root cause of the ‘damaged immune system’ theory is the misinterpretation of scientific knowledge combined with social media allowing that misinterpretation to spread easily and quickly.
Here is a Twitter thread from Dr. Jeff Gilchrist linking dozens of studies that claim various things: missing naïve T-cells, exhausted T-cells, loss of B-cell maturation, hyper-activated inflammatory response, chronic immunological dysfunction, depletion and dysfunction of dendritic cells, impaired ability to fight fungal infection, unprecedented autoimmunity.
I’ll even directly link some of studies:
Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nature Immunology 2022.
Impaired function and delayed regeneration of dendritic cells in COVID-19. PLOS Pathogens 2022.
FcγR-mediated SARS-CoV-2 infection of monocytes activates inflammation. Nature 2022.
Now, I don’t believe that any of these studies are “wrong.” In fact, some are quite good. Moreover, as I’ve said on Twitter, I’m certain that there are rare individuals that do have chronic immune damage from COVID-19. Lymphopenia (low numbers of lymphocytes, which are important immune cells) has been correlated with severe COVID-19 since March 2020!
But if millions of people had damaged T cells and damaged B cells and damaged dendritic cells and damaged monocytes, we would be seeing larger-than-normal waves of all types of infectious disease. And we aren’t.
Where people are misinterpreting is that there is a very large and meaningful difference between *statistically significant* results with ultra-precise scientific instruments and *clinically significant* impacts at the population level.
Think about it this way: by the time a drug or treatment enters Phase III clinical trials, there are mountains of data supporting its effectiveness: vast quantities of pre-clinical in silico and in vitro experiments, dozens of pre-clinical in vivo experiments likely in several different animal models (mice, rats, dogs, pigs, primates, etc.), positive Phase I and Phase II clinical trials in humans, and all of this data has been reviewed by hundreds of scientists several times over.
Yet Phase III trials fail all the time.
To use a more specific example, last week, “Transcriptional reprogramming from innate immune functions to a pro-thrombotic signature by monocytes in COVID-19” was published in Nature Communications. It went viral on social media with claims that mild COVID-19 causes blood clots.
Again, it’s a fine study that is a valuable contribution to the literature. But our advanced scientific instrumentation being able to measure minuscule changes in RNA expression or protein surface markers shouldn’t be translated into clinical outcomes. Just as picograms of mRNA in breast milk is clinically meaningless and micrograms of cocaine on every bill of US currency don’t get you high.
If you’d like to discuss blood clotting after mild COVID-19, we have that data from clinical epidemiological studies! If not fully vaccinated, your risk venous thromboembolism increases from ~0.001 to ~0.006 (top) and if fully vaccinated, there is essentially no increase (bottom)!
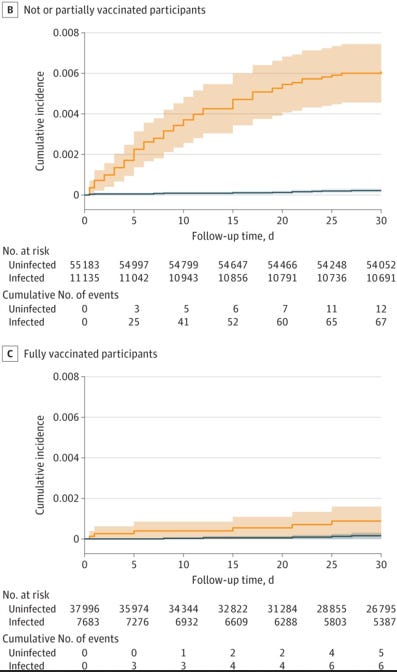
Now, does mild COVID-19 cause blood clots? In the technical sense, sure. 0.001 to 0.006 is indeed a statistically significant relative increase. But I don’t think most people live there life saying that X causes Y when the absolute incidence is 0.006.
Small statistically significant changes with ultra-precise scientific instruments are not the same thing as clinically meaningful findings at the population level. There is currently no epidemiology that indicates widespread immune damage in the broad population.
Our immune systems are fine.
Please maintain up-to-date vaccinations, focus on ventilation for airborne disease, hand-washing and surface sanitization for contact diseases, and take proper precautions for sexually-transmitted diseases.
Or depending on your media environment, that the COVID-19 vaccines damage your immune system. Regardless of your perspective, my argument is the same.
Lots and lots of assumptions by a self-described "generalist" from a 30,000 foot view using preliminary (early) 2022-2023 season data to make seemingly overly confident generalizations, none of which have been reviewed or checked by epidemiological or immunological specialists. For example, 2022-2023 flu season has barely even started and you have no way of knowing what influenza hospitalization numbers will be a month from now or 3 months from now. Yet you already feel confident enough to declare the surprisingly early influenza wave we're seeing will end suddenly and no more for the several months remaining in the season, so for 2023, "all signs suggest it is normal in magnitude and severity." Wow. Do you know where one can procure a crystal ball like the one you apparently have?
At least allow me to suggest the title should perhaps be re-written with a little less hasty certitude and finality as such:
̶O̶u̶r̶ ̶I̶m̶m̶u̶n̶e̶ ̶S̶y̶s̶t̶e̶m̶s̶ ̶W̶e̶r̶e̶n̶'̶t̶ ̶D̶a̶m̶a̶g̶e̶d̶ ̶b̶y̶ ̶S̶A̶R̶S̶-̶C̶o̶V̶-̶2̶
If Our Immune Systems Were Damaged, I'm Not Yet Seeing Significant Increases In Frequency/Morbidity Of Regular Disease Or Opportunistic Infections
And, I might suggest you reach out to some experts/specialists to double check some of your numerous assumptions.